

Gene-based Confirmatory Germline Testing Following Tumor-only Sequencing of Prostate Cancer
- PMID: 36115772
- PMCID: PMC10208030
- DOI: 10.1016/j.eururo.2022.08.028
Gene-based Confirmatory Germline Testing Following Tumor-only Sequencing of Prostate Cancer
Abstract
Background: Tumor-only genomic profiling is an important tool in therapeutic management of men with prostate cancer. Since clinically actionable germline variants may be reflected in tumor profiling, it is critical to identify which variants have a higher risk of being germline in origin to better counsel patients and prioritize genetic testing.
Objective: To determine when variants found on tumor-only sequencing of prostate cancers should prompt confirmatory germline testing.
Design, setting, and participants: Men with prostate cancer who underwent both tumor and germline sequencing at Memorial Sloan Kettering Cancer Center from January 1, 2015 to January 31, 2020 were evaluated.
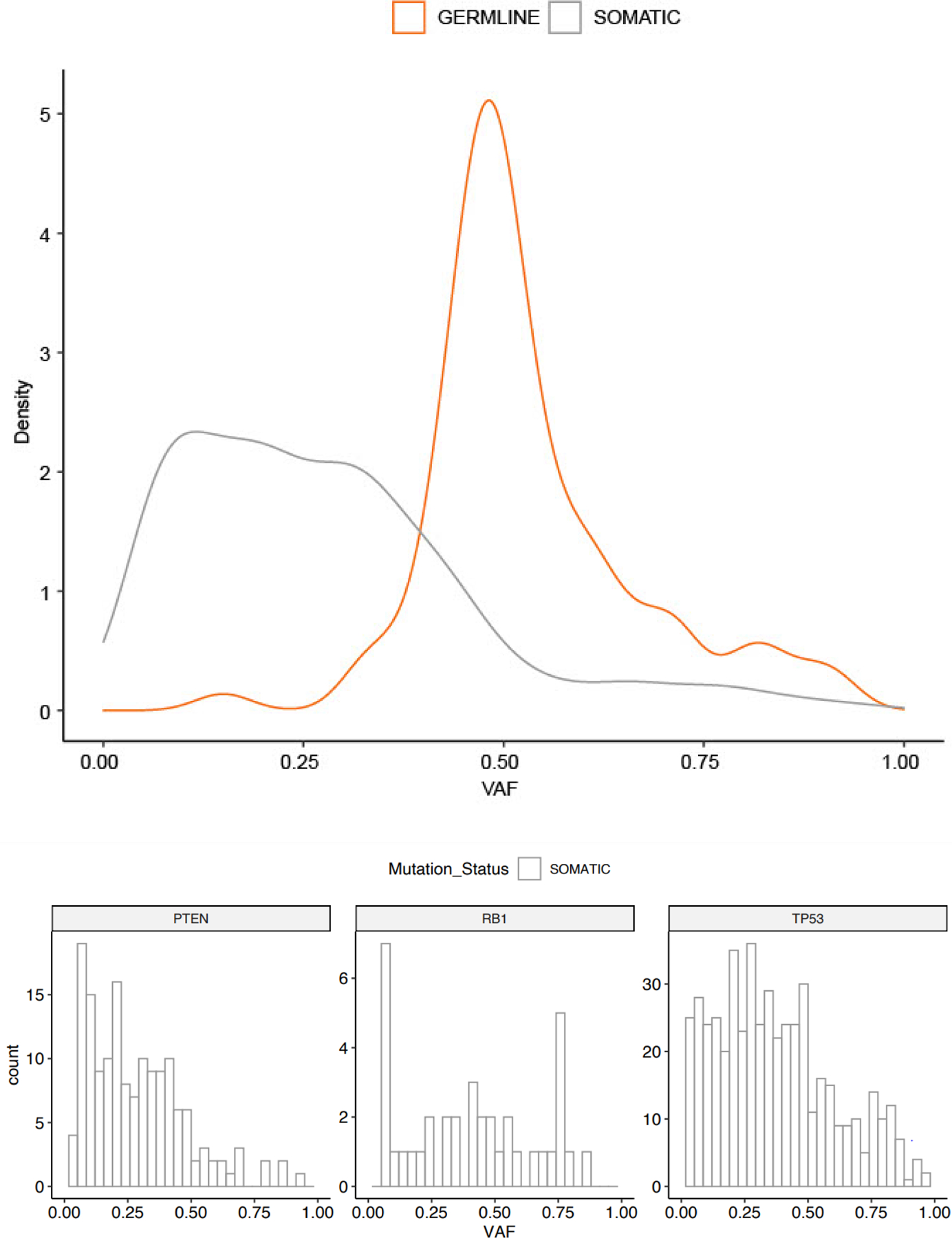
Outcome measurements and statistical analysis: Tumor and germline profiles were analyzed for pathogenic and likely pathogenic ("pathogenic") variants in 60 moderate- or high-penetrance genes associated with cancer predisposition. The germline probability (germline/germline + somatic) of a variant was calculated for each gene. Clinical and pathologic factors were analyzed as potential modifiers of germline probability.
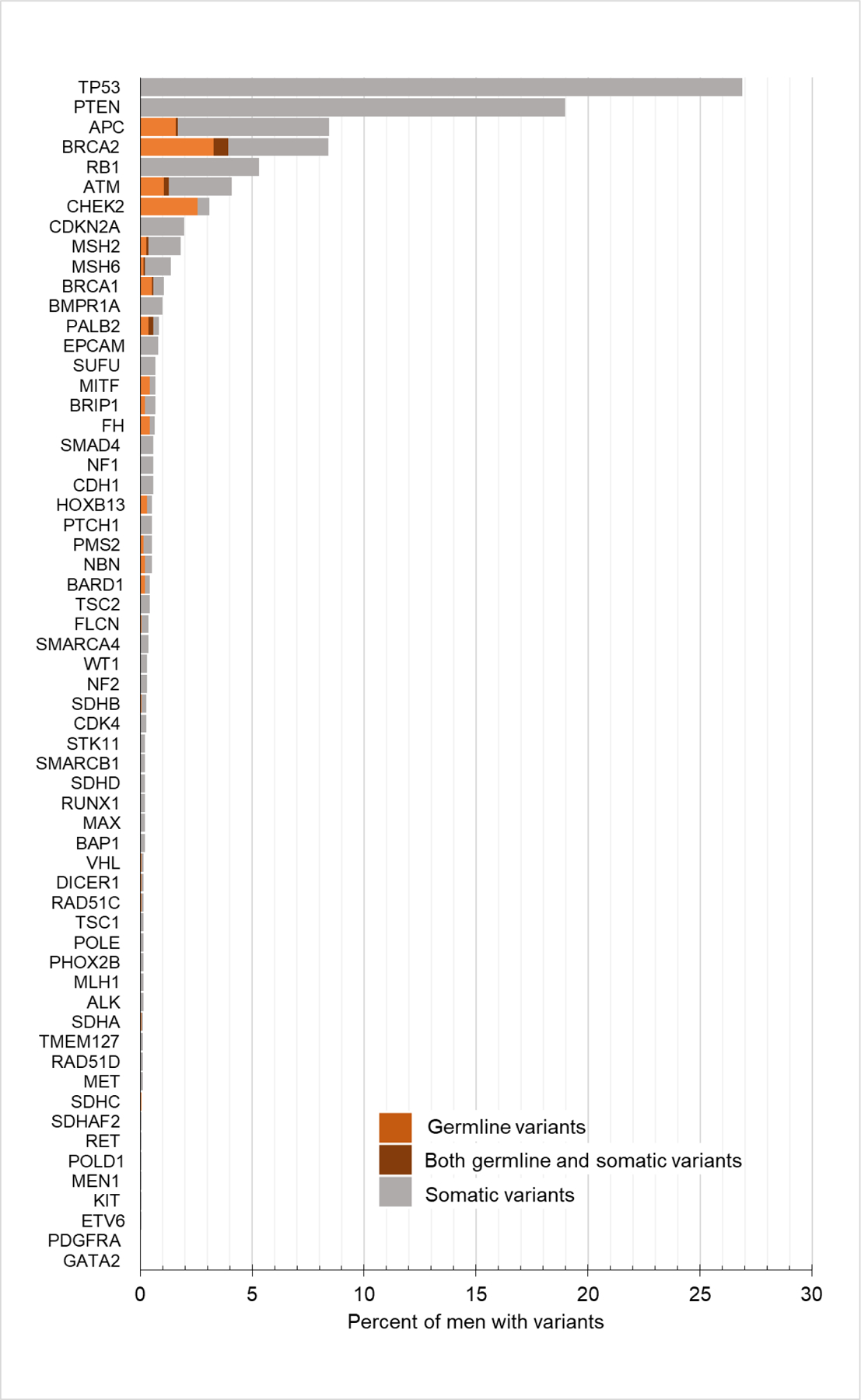
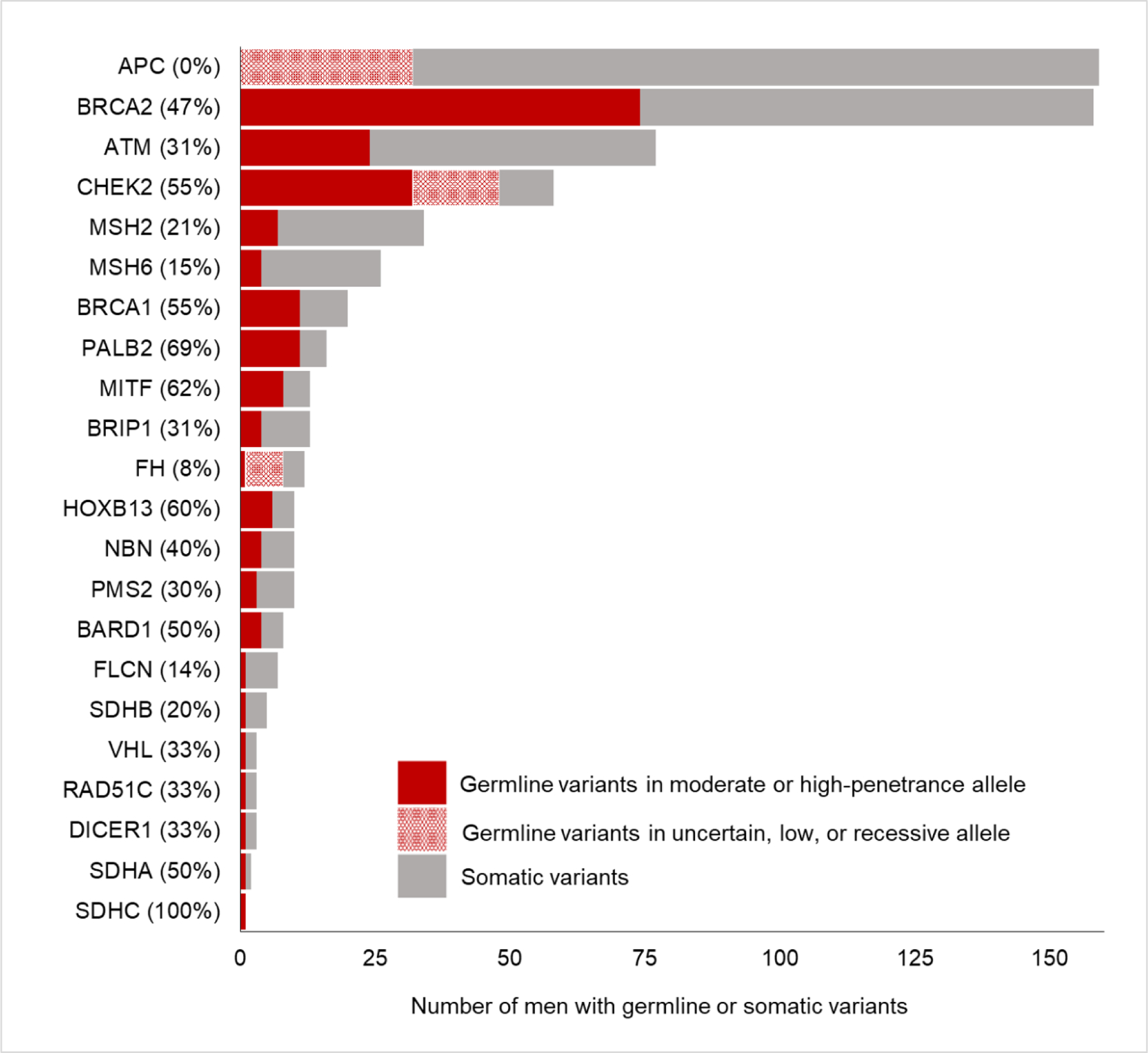
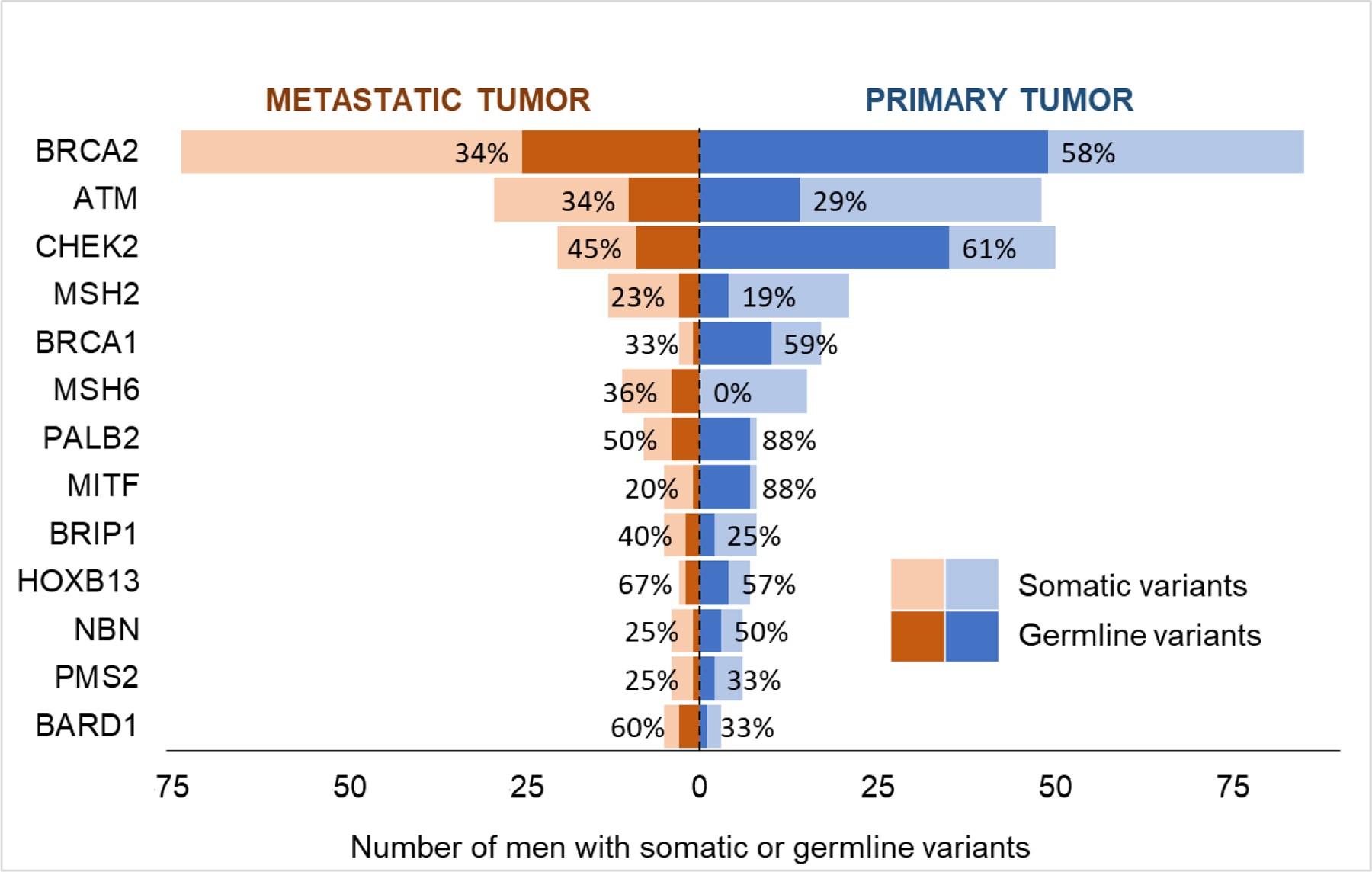
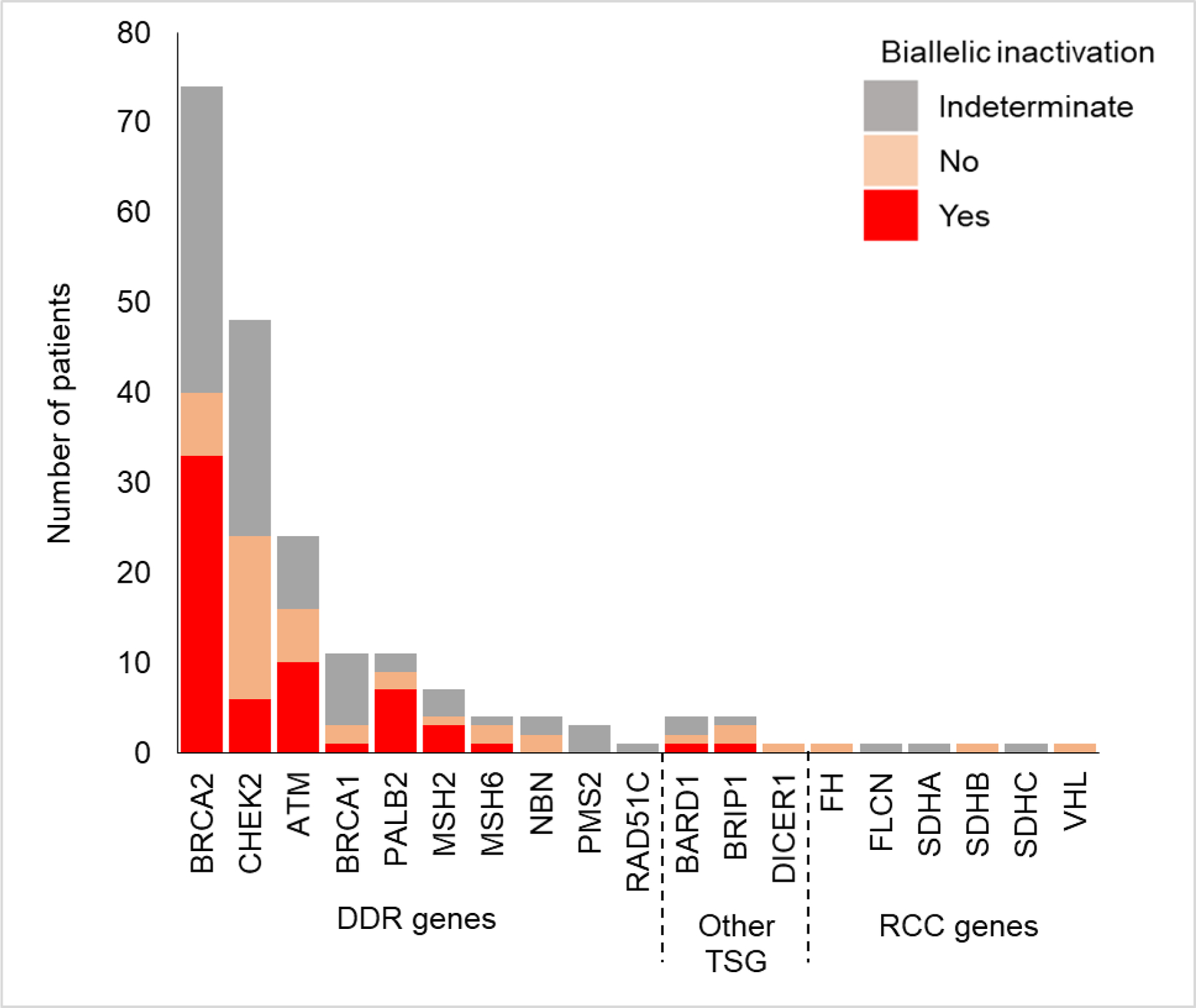
Results and limitations: Of the 1883 patients identified, 1084 (58%) had a somatic or germline pathogenic variant in one of 60 cancer susceptibility genes, and of them, 240 (22%) had at least one germline variant. Overall, the most frequent variants were in TP53, PTEN, APC, BRCA2, RB1, ATM, and CHEK2. Variants in TP53, PTEN, or RB1 were identified in 746 (40%) patients and were exclusively somatic. Variants with the highest germline probabilities were in PALB2 (69%), MITF (62%), HOXB13 (60%), CHEK2 (55%), BRCA1 (55%), and BRCA2 (47%), and the overall germline probability of a variant in any DNA damage repair gene was 40%. Limitations were that most of the men included in the cohort had metastatic disease, and different thresholds for pathogenicity exist for somatic and germline variants.
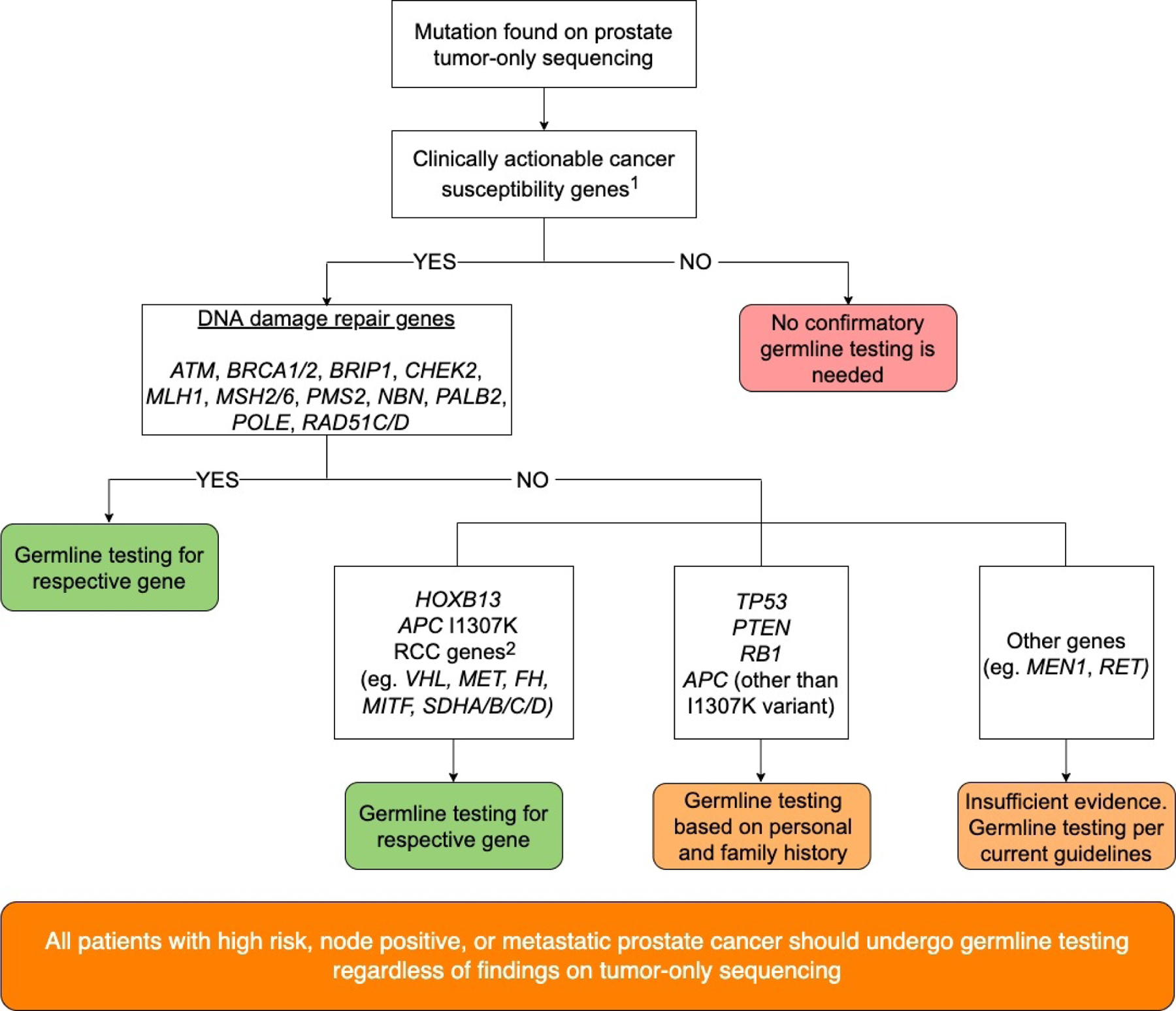
Conclusions: Of patients with pathogenic variants found on prostate tumor sequencing, 22% had clinically actionable germline variants, for which the germline probabilities varied widely by gene. Our results provide an evidenced-based clinical framework to prioritize referral to genetic counseling following tumor-only sequencing.
Patient summary: Patients with advanced prostate cancer are recommended to have germline genetic testing. Genetic sequencing of a patient's prostate tumor may also identify certain gene variants that are inherited. We found that patients who had variants in certain genes, such as ones that function in DNA damage repair, identified in their prostate tumor sequencing, had a high risk for having an inherited cancer syndrome.
Keywords: Advanced prostate cancer; DNA damage repair genes; Germline testing; Tumor-only sequencing.
Copyright © 2022 European Association of Urology. Published by Elsevier B.V. All rights reserved.
Conflict of interest statement
Figures
References
-
- National Comprehensive Cancer Network. Prostate cancer (version 2.2021)
-
- De Bono J, Mateo J, Fizazi K, et al. Olaparib for metastatic castration-resistant prostate cancer. N Engl J Med 2020;382:2091–102. - PubMed
-
- Clarke N, Wiechno P, Alekseev B, et al. Olaparib combined with abiraterone in patients with metastatic castration-resistant prostate cancer: a randomised, double-blind, placebo-controlled, phase 2 trial. Lancet Oncol 2018;19:975–86. - PubMed
-
- Evans DG, Susnerwala I, Dawson J, Woodward E, Maher ER, Lalloo F. Risk of breast cancer in male BRCA2 carriers. J Med Genet 2010;47:710–1. - PubMed
MeSH terms
Grants and funding
LinkOut - more resources
Full Text Sources
Medical
Research Materials
Miscellaneous
