

Ischemia With Nonobstructive Coronary Arteries: Insights From the ISCHEMIA Trial
- PMID: 36115814
- PMCID: PMC9878463
- DOI: 10.1016/j.jcmg.2022.06.015
Ischemia With Nonobstructive Coronary Arteries: Insights From the ISCHEMIA Trial
Abstract
Background: Ischemia with nonobstructive coronary arteries (INOCA) is common clinically, particularly among women, but its prevalence among patients with at least moderate ischemia and the relationship between ischemia severity and non-obstructive atherosclerosis severity are unknown.
Objectives: The authors investigated predictors of INOCA in enrolled, nonrandomized participants in ISCHEMIA (International Study of Comparative Health Effectiveness with Medical and Invasive Approaches), sex differences, and the relationship between ischemia and atherosclerosis in patients with INOCA.
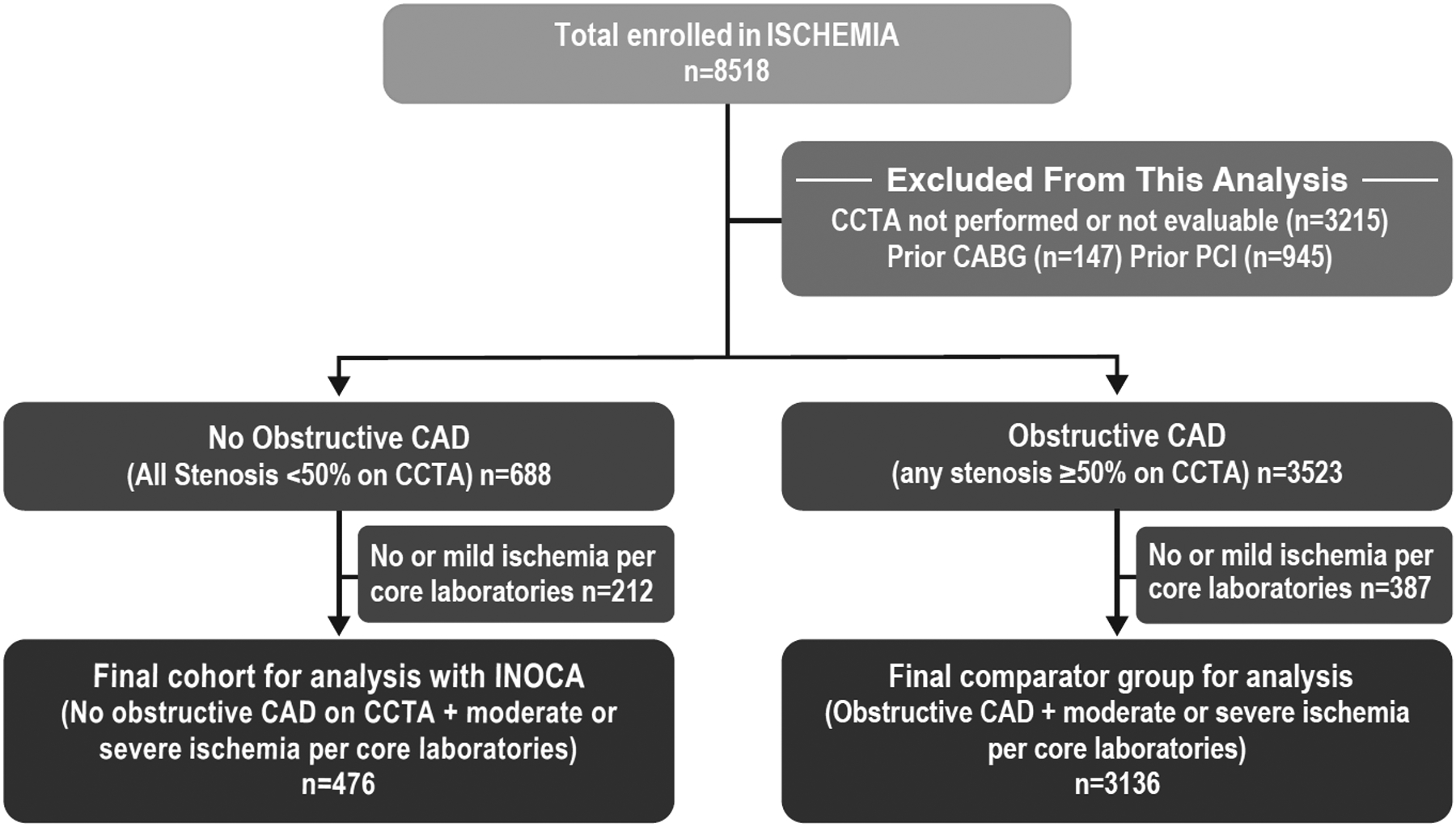
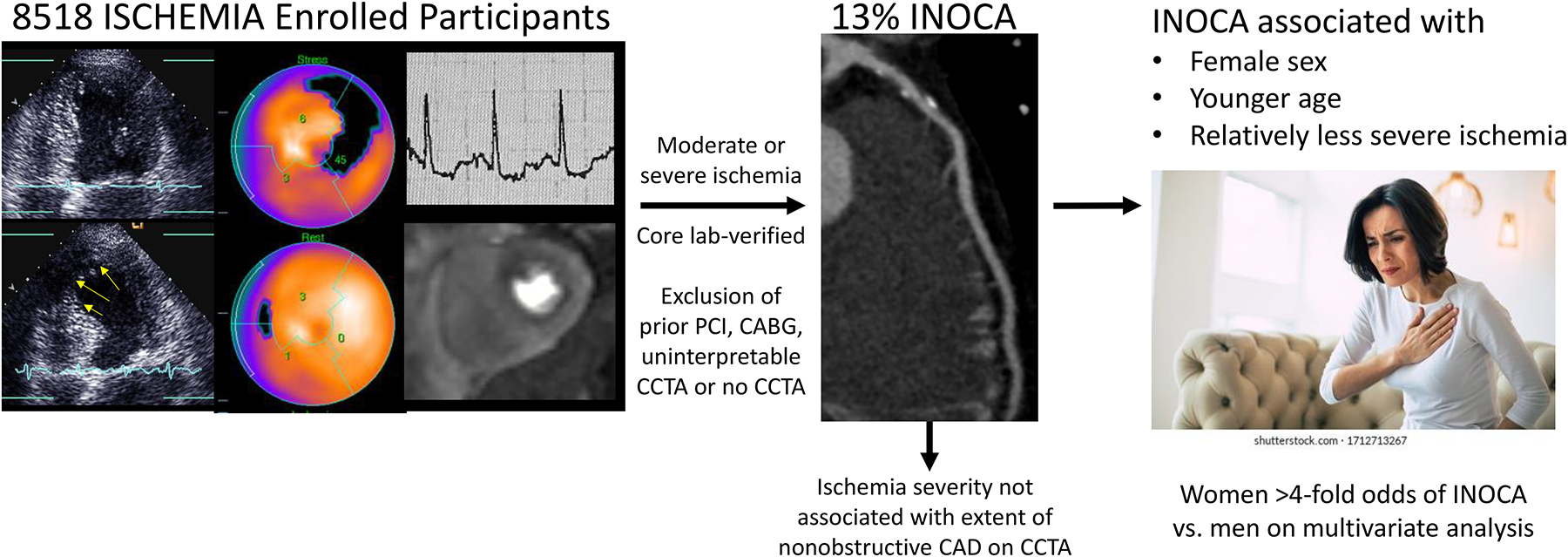
Methods: Core laboratories independently reviewed screening noninvasive stress test results (nuclear imaging, echocardiography, magnetic resonance imaging or nonimaging exercise tolerance testing), and coronary computed tomography angiography (CCTA), blinded to results of the screening test. INOCA was defined as all stenoses <50% on CCTA in a patient with moderate or severe ischemia on stress testing. INOCA patients, who were excluded from randomization, were compared with randomized participants with ≥50% stenosis in ≥1 vessel and moderate or severe ischemia.
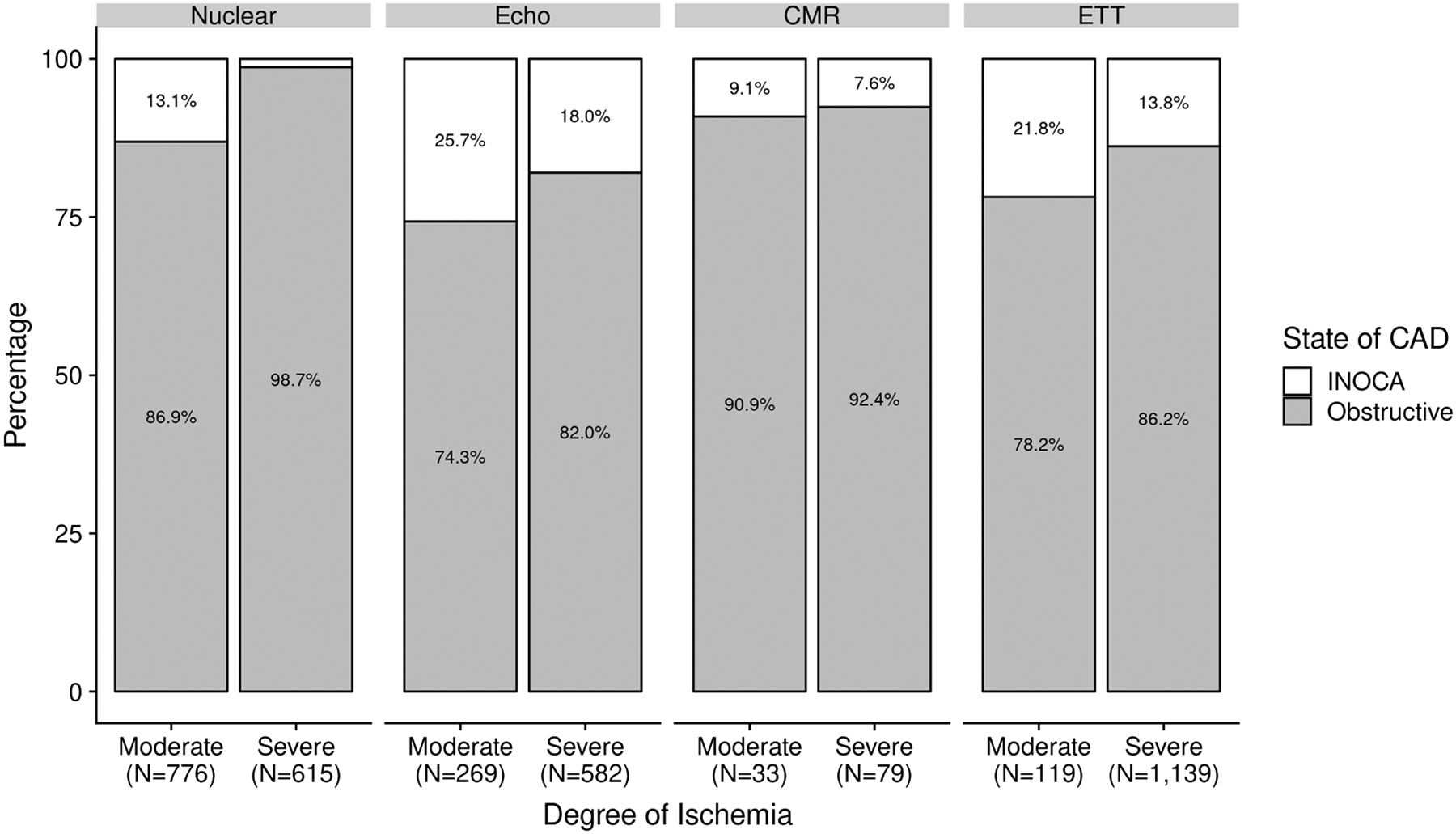
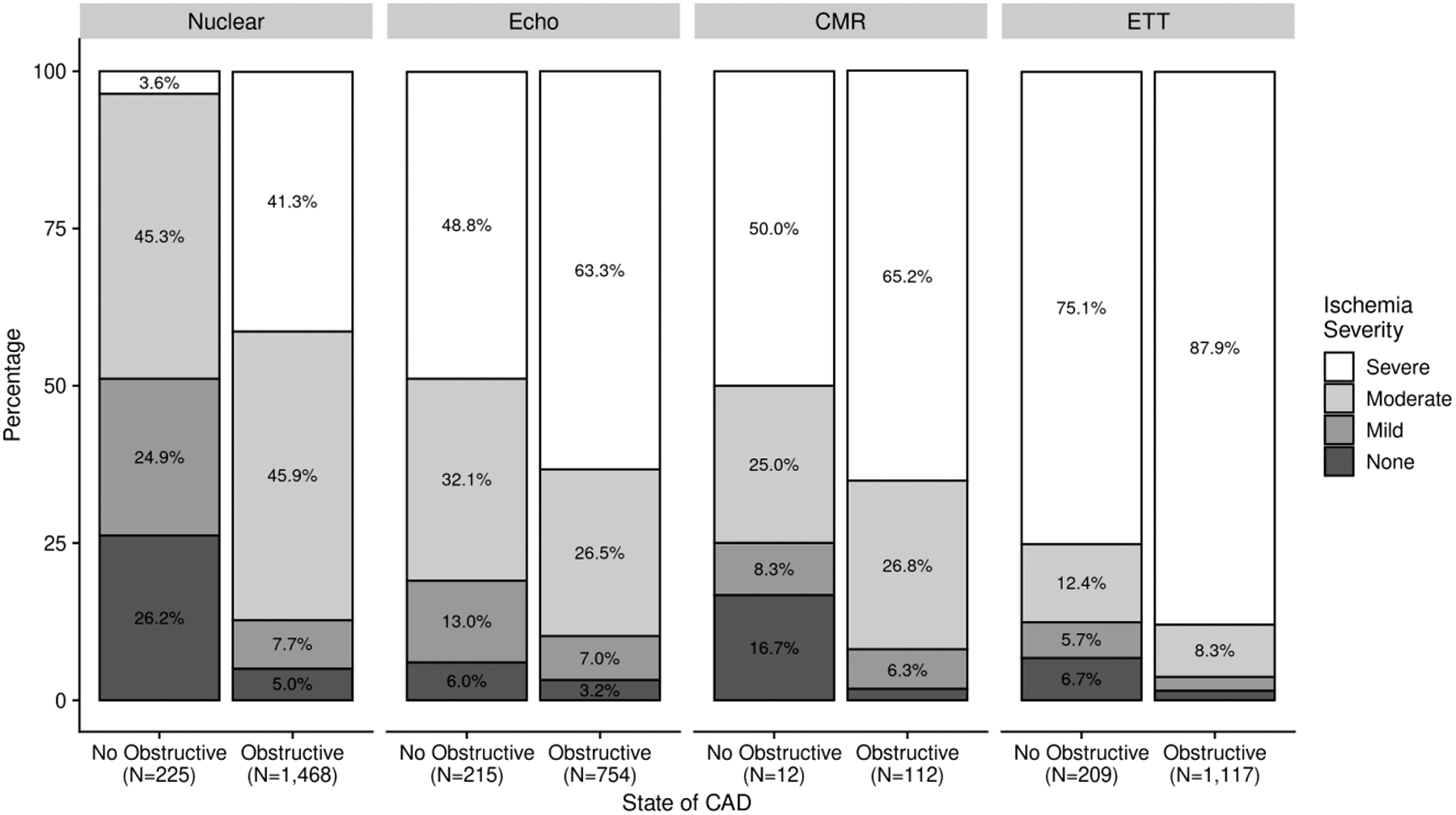
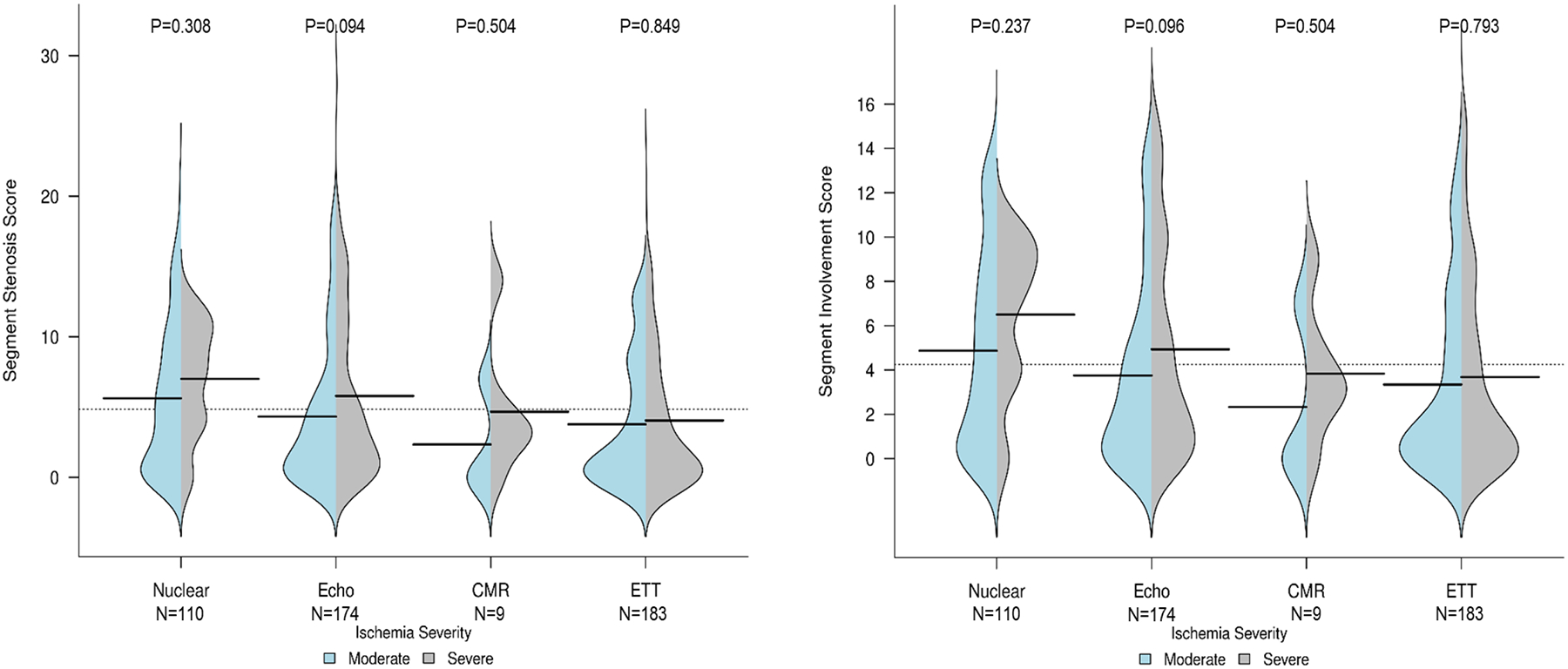
Results: Among 3,612 participants with core laboratory-confirmed moderate or severe ischemia and interpretable CCTA, 476 (13%) had INOCA. Patients with INOCA were younger, were predominantly female, and had fewer atherosclerosis risk factors. For each stress testing modality, the extent of ischemia tended to be less among patients with INOCA, particularly with nuclear imaging. There was no significant relationship between severity of ischemia and extent or severity of nonobstructive atherosclerosis on CCTA. On multivariable analysis, female sex was independently associated with INOCA (odds ratio: 4.2 [95% CI: 3.4-5.2]).
Conclusions: Among participants enrolled in ISCHEMIA with core laboratory-confirmed moderate or severe ischemia, the prevalence of INOCA was 13%. Severity of ischemia was not associated with severity of nonobstructive atherosclerosis. (International Study of Comparative Health Effectiveness With Medical and Invasive Approaches [ISCHEMIA]; NCT01471522).
Keywords: coronary CT angiography; ischemia; ischemia with nonobstructive coronary arteries; stress testing.
Copyright © 2023 The Authors. Published by Elsevier Inc. All rights reserved.
Conflict of interest statement
Funding Support and Author Disclosures This project was supported by National Institutes of Health grants (U01HL105907, U01HL105462, U01HL105561, and U01HL105565) and supported in part by Clinical Translational Science Award (11UL1 TR001445 and UL1 TR002243) from the National Center for Advancing Translational Sciences and by grants from Arbor Pharmaceuticals LLC and AstraZeneca Pharmaceuticals LP. The manuscript contents are solely the responsibility of the authors and do not necessarily represent official views of the National Center for Advancing Translational Sciences, the National Heart, Lung, and Blood Institute, the National Institutes of Health, or the Department of Health and Human Services. Devices or medications were provided by Abbott Vascular (previously St. Jude Medical, Inc); Medtronic, Inc; Phillips (previously Volcano Corporation); and Omron Healthcare, Inc; medications were provided by Amgen Inc; Arbor Pharmaceuticals, LLC; AstraZeneca Pharmaceuticals, LP; Espero Pharmaceuticals; Merck, Sharp & Dohme Corp; and Sunovion Pharmaceuticals. All authors have received funding from the National Heart, Lung and Blood Institute for the study. Dr Reynolds has received nonfinancial support from Abbott Vascular, Siemens, BioTelemetry, and Leipsic; is a consultant and holder of stock options from Circle CVI and HeartFlow; is the recipient of research grants from GE Healthcare and Edwards; and serves on speakers bureaus for Philips and GE Healthcare. Dr Budoff has received grant support from General Electric; has been on the Medical Advisory Board of Arineta; and has received salary from and has ownership interest in Cleerly, Inc. Dr Berman has received software royalties from Cedars-Sinai Medical Center. Dr Lopes has received grants and other support from Bayer, Boehringer Ingleheim, Bristol-Myers Squibb, Daiichi Sankyo, and Glaxo Smith Kline; and has received grants from Medtronic, Merck, Pfizer, Portola, and Sanofi. Dr Chow holds the Saul and Edna Goldfarb Chair in Cardiac Imaging Research; has received research support from TD Bank, CV Diagnostix and AusculSciences, and Siemens Healthineers; and has equity interest in General Electric. Dr Stone has received personal fees from Terumo, Amaranth, Shockwave, Valfix, TherOx, Reva, Vascular Dynamics, Robocath, HeartFlow, Gore, Ablative Solutions, Matrizyme, Miracor, Neovasc, V-wave, SpectreWave, MAIA Pharmaceuticals, Orchestra Biomed, Vectorious Abiomed, Claret, Sirtex, Ancora, and Qool Therapeutics; other considerations from Cagent, Applied Therapeutics, Biostar family of funds; support from MedFocus family of funds, Aria; and personal fees from Cardiac Success work. Dr Boden has received support from Abbvie and Amarin; grants from Amgen; and personal fees from Amgen, Cleveland Clinic Clinical Coordinating Center, and Janssen. Dr Bangalore has received grants and personal fees from Abbott Vascular; and personal fees from Biotronik, Pfizer, and Amgen. Dr Hochman is principal investigator for the ISCHEMIA trial, for which grant, devices, and medications were provided by Abbott Vascular; Medtronic, Inc; St. Jude Medical, Inc; Volcano Corporation; Arbor Pharmaceuticals, LLC; AstraZeneca Pharmaceuticals, LP; Merck Sharp & Dohme Corp; Omron Healthcare, Inc; and financial donations from Arbor Pharmaceuticals LLC and AstraZeneca Pharmaceuticals LP.
Figures
Comment in
-
ISCHEMIA Sheds Light on INOCA: Understanding Population Heterogeneity to Inform Prognosis and Guide Management.JACC Cardiovasc Imaging. 2023 Jan;16(1):75-77. doi: 10.1016/j.jcmg.2022.10.012. JACC Cardiovasc Imaging. 2023. PMID: 36599571 No abstract available.
References
-
- Kunadian V, Chieffo A, Camici PG et al. An EAPCI Expert Consensus Document on Ischaemia with Non-Obstructive Coronary Arteries in Collaboration with European Society of Cardiology Working Group on Coronary Pathophysiology & Microcirculation Endorsed by Coronary Vasomotor Disorders International Study Group. European Heart Journal 2020;41:3504–3520. - PMC - PubMed
