

Low Cardiorespiratory Fitness Post-COVID-19: A Narrative Review
- PMID: 36115933
- PMCID: PMC9483283
- DOI: 10.1007/s40279-022-01751-7
Low Cardiorespiratory Fitness Post-COVID-19: A Narrative Review
Abstract
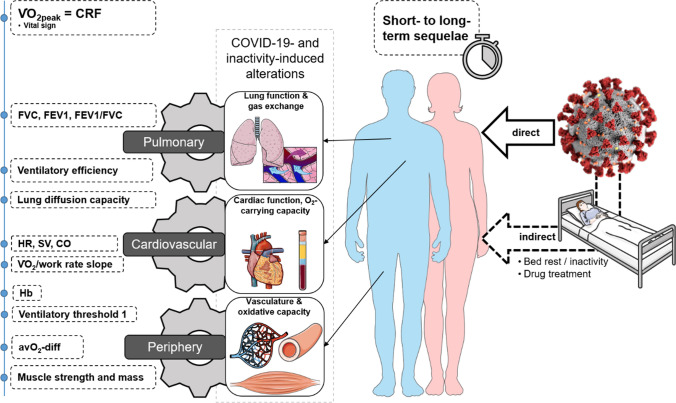
Patients recovering from COVID-19 often report symptoms of exhaustion, fatigue and dyspnoea and present with exercise intolerance persisting for months post-infection. Numerous studies investigated these sequelae and their possible underlying mechanisms using cardiopulmonary exercise testing. We aimed to provide an in-depth discussion as well as an overview of the contribution of selected organ systems to exercise intolerance based on the Wasserman gears. The gears represent the pulmonary system, cardiovascular system, and periphery/musculature and mitochondria. Thirty-two studies that examined adult patients post-COVID-19 via cardiopulmonary exercise testing were included. In 22 of 26 studies reporting cardiorespiratory fitness (herein defined as peak oxygen uptake-VO2peak), VO2peak was < 90% of predicted value in patients. VO2peak was notably below normal even in the long-term. Given the available evidence, the contribution of respiratory function to low VO2peak seems to be only minor except for lung diffusion capacity. The prevalence of low lung diffusion capacity was high in the included studies. The cardiovascular system might contribute to low VO2peak via subnormal cardiac output due to chronotropic incompetence and reduced stroke volume, especially in the first months post-infection. Chronotropic incompetence was similarly present in the moderate- and long-term follow-up. However, contrary findings exist. Peripheral factors such as muscle mass, strength and perfusion, mitochondrial function, or arteriovenous oxygen difference may also contribute to low VO2peak. More data are required, however. The findings of this review do not support deconditioning as the primary mechanism of low VO2peak post-COVID-19. Post-COVID-19 sequelae are multifaceted and require individual diagnosis and treatment.
© 2022. The Author(s).
Conflict of interest statement
Fabian Schwendinger, Raphael Knaier, Thomas Radtke and Arno Schmidt-Trucksäss declare that they have no conflicts of interest relevant to the content of this review.
Figures

References
-
- Gebhard CE, Sütsch C, Bengs S, Deforth M, Buehler KP, Hamouda N, et al. Sex- and gender-specific risk factors of post-COVID-19 Syndrome: a population-based cohort study in Switzerland. medRxiv. 2021:2021.06.30.21259757.
-
- Kuodi P, Gorelik Y, Zayyad H, Wertheim O, Wiegler KB, Jabal KA, et al. Association between vaccination status and reported incidence of post-acute COVID-19 symptoms in Israel: a cross-sectional study of patients infected between March 2020 and November 2021. medRxiv. 2022:2022.01.05.22268800.
Publication types
MeSH terms
Substances
Grants and funding
LinkOut - more resources
Full Text Sources
Medical
