

Hyperthermic intraperitoneal chemotherapy (HIPEC) for the management of primary advanced and recurrent ovarian cancer: a systematic review and meta-analysis of randomized trials
- PMID: 36116421
- PMCID: PMC9588894
- DOI: 10.1016/j.esmoop.2022.100586
Hyperthermic intraperitoneal chemotherapy (HIPEC) for the management of primary advanced and recurrent ovarian cancer: a systematic review and meta-analysis of randomized trials
Abstract
Introduction: Ovarian cancer is the most lethal gynecologic malignancy. Although treatment with hyperthermic intraperitoneal chemotherapy (HIPEC) has shown promising results, its role remains elusive. The aim of this study was to assess the comprehensive randomized evidence for the use versus non-use of HIPEC in primary and recurrent ovarian cancer.
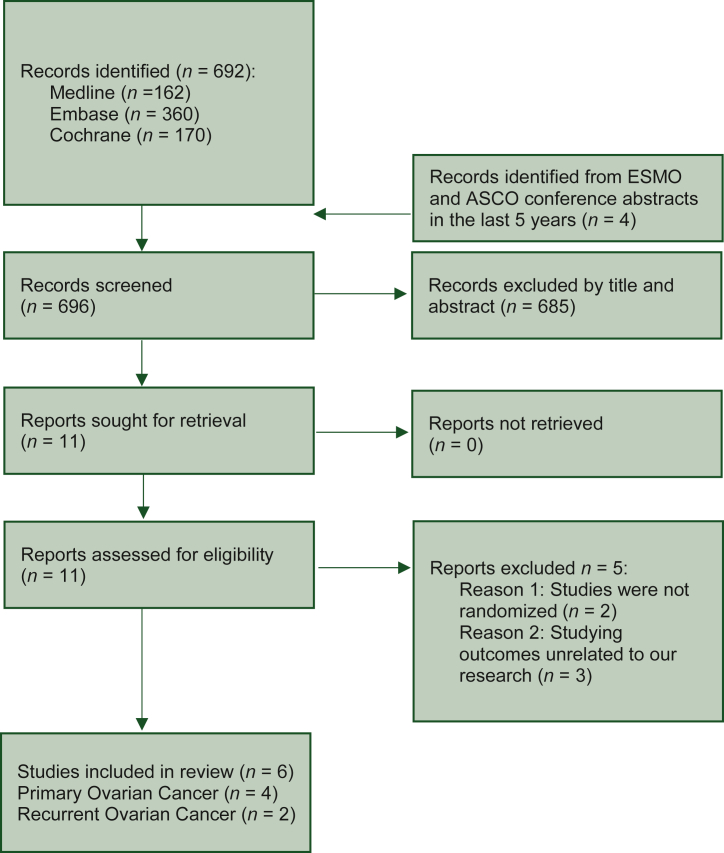
Materials and methods: The Medline, Embase and Cochrane databases, as well as the European Society for Medical Oncology (ESMO) and American Society of Clinical Oncology (ASCO) conference abstracts of the last 5 years, were scrutinized in January 2022 for randomized, controlled trials that studied the use of HIPEC in ovarian cancer. Overall survival (OS), disease-free survival (DFS) and progression-free survival, as well as post-operative morbidity were the outcomes of interest. This study was reported in accordance with the Preferred Reporting Items for Systematic Reviews and Meta-Analyses (PRISMA) reporting guideline.
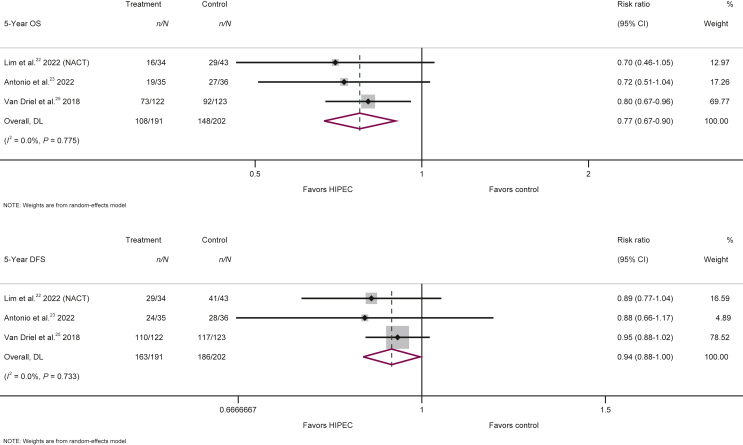
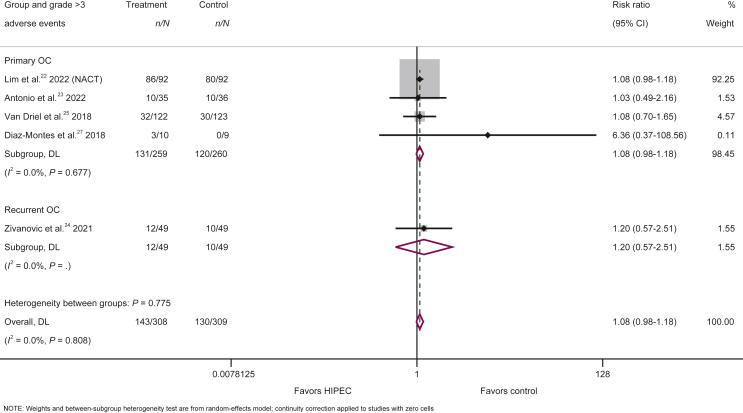
Results: Six randomized, controlled trials that randomized 737 patients were included in our analysis; of these, four studies (519 patients) were in primary and two (218 patients) in recurrent settings. In primary ovarian cancer, the combination of HIPEC with interval cytoreductive surgery (CRS) and neoadjuvant chemotherapy significantly improved the 5-year OS [393 patients, risk ratio (RR) = 0.77; 95% confidence interval (CI) 0.67-0.90; P value = 0.001] and DFS (hazard ratio = 0.60; 95% CI 0.41-0.87; P value = 0.008) compared with standard treatment alone. In the absence of neoadjuvant chemotherapy, the use of HIPEC + CRS was not associated with any survival advantage (126 patients, 4-year OS, RR = 0.93; 95% CI 0.57-1.53; P value = 0.781), but the sample size was smaller in this subset. Use of HIPEC in recurrent ovarian cancer did not provide any survival advantage (5-year OS: 218 patients, RR = 0.85; 95% CI 0.45-1.62; P value = 0.626). The risk for grade ≥3 adverse events was similar between HIPEC and no HIPEC (RR = 1.08; 95% CI 0.98-1.18; P value = 0.109).
Conclusions: In primary ovarian cancer the combination of HIPEC with interval CRS and neoadjuvant chemotherapy is a safe option that significantly improved 5-year OS and DFS. Its use in other settings should continue to be considered investigational.
Keywords: HIPEC; cytoreductive surgery; hyperthermic intraperitoneal chemotherapy; interval CRS; ovarian cancer; primary CRS.
Copyright © 2022 The Author(s). Published by Elsevier Ltd.. All rights reserved.
Conflict of interest statement
Disclosure The authors have declared no conflicts of interest. Data sharing All data generated or analysed during this study are included in this published article (and its supplementary information files).
Figures
References
-
- Siegel R.L., Miller K.D., Fuchs H.E., Jemal A. Cancer statistics, 2022. CA Cancer J Clin. 2022;72(1):7–33. - PubMed
-
- Siegel R.L., Miller K.D., Jemal A. Cancer statistics, 2016. CA Cancer J Clin. 2016;66(1):7–30. - PubMed
-
- Meigs J.V. The Macmillan Company; New York: 1934. Tumors of the Female Pelvic Organs.
-
- Griffiths C.T. Surgical resection of tumor bulk in the primary treatment of ovarian carcinoma. Natl Cancer Inst Monogr. 1975;42:101–104. - PubMed
-
- Hoskins W.J., Bundy B.N., Thigpen J.T., Omura G.A. The influence of cytoreductive surgery on recurrence-free interval and survival in small-volume stage III epithelial ovarian cancer: a Gynecologic Oncology Group study. Gynecol Oncol. 1992;47(2):159–166. - PubMed
Publication types
MeSH terms
LinkOut - more resources
Full Text Sources
Medical
