

Cost-effectiveness of strategies to control the spread of carbapenemase-producing Enterobacterales in hospitals: a modelling study
- PMID: 36117231
- PMCID: PMC9484055
- DOI: 10.1186/s13756-022-01149-0
Cost-effectiveness of strategies to control the spread of carbapenemase-producing Enterobacterales in hospitals: a modelling study
Abstract
Background: Spread of resistant bacteria causes severe morbidity and mortality. Stringent control measures can be expensive and disrupt hospital organization. In the present study, we assessed the effectiveness and cost-effectiveness of control strategies to prevent the spread of Carbapenemase-producing Enterobacterales (CPE) in a general hospital ward (GW).
Methods: A dynamic, stochastic model simulated the transmission of CPE by the hands of healthcare workers (HCWs) and the environment in a hypothetical 25-bed GW. Input parameters were based on published data; we assumed the prevalence at admission of 0.1%. 12 strategies were compared to the baseline (no control) and combined different prevention and control interventions: targeted or universal screening at admission (TS or US), contact precautions (CP), isolation in a single room, dedicated nursing staff (DNS) for carriers and weekly screening of contact patients (WSC). Time horizon was one year. Outcomes were the number of CPE acquisitions, costs, and incremental cost-effectiveness ratios (ICER). A hospital perspective was adopted to estimate costs, which included laboratory costs, single room, contact precautions, staff time, i.e. infection control nurse and/or dedicated nursing staff, and lost bed-days due to prolonged hospital stay of identified carriers. The model was calibrated on actual datasets. Sensitivity analyses were performed.
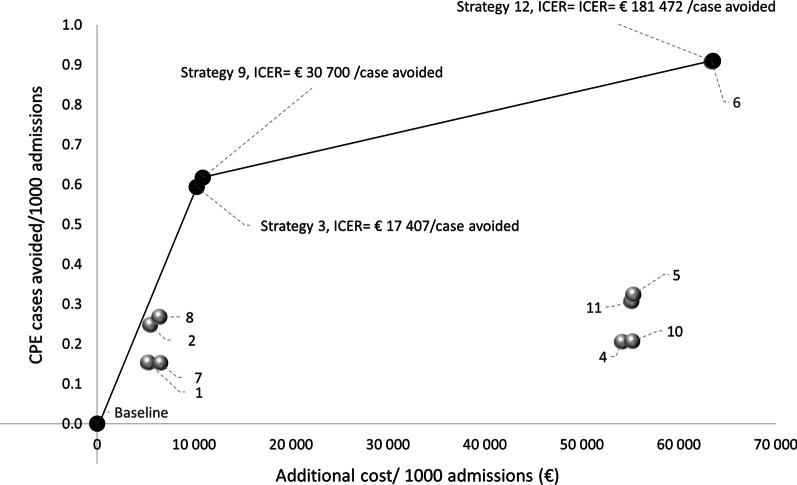
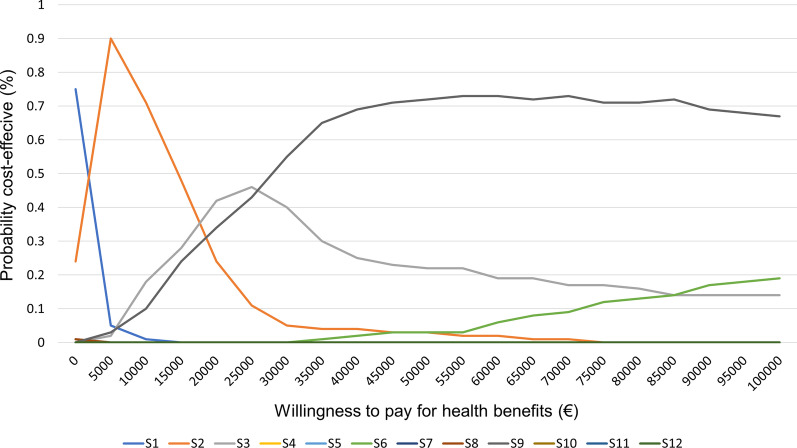
Results: The baseline scenario resulted in 0.93 CPE acquisitions/1000 admissions and costs 32,050 €/1000 admissions. All control strategies increased costs and improved the outcome. The efficiency frontier was represented by: (1) TS with DNS at a 17,407 €/avoided CPE case, (2) TS + DNS + WSC at a 30,700 €/avoided CPE case and (3) US + DNS + WSC at 181,472 €/avoided CPE case. Other strategies were dominated. Sensitivity analyses showed that TS + CP might be cost-effective if CPE carriers are identified upon admission or if the cases have a short hospital stay. However, CP were effective only when high level of compliance with hand hygiene was obtained.
Conclusions: Targeted screening at admission combined with DNS for identified CPE carriers with or without weekly screening were the most cost-effective options to limit the spread of CPE. These results support current recommendations from several high-income countries.
Keywords: Carbapenemase-producing Enterobacterales; Control strategies; Cost-effectiveness; Cross-transmission; France; Hand disinfection; Mathematical model.
© 2022. The Author(s).
Conflict of interest statement
All authors declare no competing interests.
Figures


References
-
- Patients: Information about CRE. 2021 [cited 2021 Dec 7]. Available from: https://www.cdc.gov/hai/organisms/cre/cre-patients.html
-
- Cassini A, Högberg LD, Plachouras D, Quattrocchi A, Hoxha A, Simonsen GS, et al. Attributable deaths and disability-adjusted life-years caused by infections with antibiotic-resistant bacteria in the EU and the European Economic Area in 2015: a population-level modelling analysis. Lancet Infect Dis. 2019;19:56–66. doi: 10.1016/S1473-3099(18)30605-4. - DOI - PMC - PubMed
-
- Magiorakos AP, Burns K, Rodríguez Baño J, Borg M, Daikos G, Dumpis U, et al. Infection prevention and control measures and tools for the prevention of entry of carbapenem-resistant Enterobacteriaceae into healthcare settings: guidance from the European Centre for Disease Prevention and Control. Antimicrob Resist Infect Control. 2017;6:113. doi: 10.1186/s13756-017-0259-z. - DOI - PMC - PubMed
-
- World Health Organization. Guidelines for the prevention and control of carbapenem-resistant Enterobacteriaceae, Acinetobacter baumannii, and Pseudomonas aeruginosa in health care facilities.. 2017 [cited 2021 Oct 1]. Available from: http://www.ncbi.nlm.nih.gov/books/NBK493061/ - PubMed
-
- Haut Conseil de la Santé Publique. Actualisation des recommandations relatives aux BHRe. 2019. Available from: https://www.hcsp.fr/Explore.cgi/avisrapportsdomaine?clefr=758
Publication types
MeSH terms
Substances
LinkOut - more resources
Full Text Sources
Research Materials
Miscellaneous
