

Anti-SARS-CoV-2 activity of targeted kinase inhibitors: Repurposing clinically available drugs for COVID-19 therapy
- PMID: 36117402
- PMCID: PMC9538324
- DOI: 10.1002/jmv.28157
Anti-SARS-CoV-2 activity of targeted kinase inhibitors: Repurposing clinically available drugs for COVID-19 therapy
Abstract
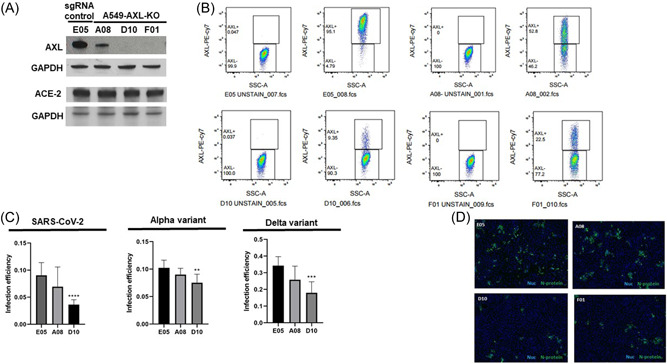
Coronavirus disease 2019 (COVID-19) remains a major public health concern, and vaccine unavailability, hesitancy, or failure underscore the need for discovery of efficacious antiviral drug therapies. Numerous approved drugs target protein kinases associated with viral life cycle and symptoms of infection. Repurposing of kinase inhibitors is appealing as they have been vetted for safety and are more accessible for COVID-19 treatment. However, an understanding of drug mechanism is needed to improve our understanding of the factors involved in pathogenesis. We tested the in vitro activity of three kinase inhibitors against severe acute respiratory syndrome coronavirus 2 (SARS-CoV-2), including inhibitors of AXL kinase, a host cell factor that contributes to successful SARS-CoV-2 infection. Using multiple cell-based assays and approaches, gilteritinib, nintedanib, and imatinib were thoroughly evaluated for activity against SARS-CoV-2 variants. Each drug exhibited antiviral activity, but with stark differences in potency, suggesting differences in host dependency for kinase targets. Importantly, for gilteritinib, the amount of compound needed to achieve 90% infection inhibition, at least in part involving blockade of spike protein-mediated viral entry and at concentrations not inducing phospholipidosis (PLD), approached a clinically achievable concentration. Knockout of AXL, a target of gilteritinib and nintedanib, impaired SARS-CoV-2 variant infectivity, supporting a role for AXL in SARS-CoV-2 infection and supporting further investigation of drug-mediated AXL inhibition as a COVID-19 treatment. This study supports further evaluation of AXL-targeting kinase inhibitors as potential antiviral agents and treatments for COVID-19. Additional mechanistic studies are needed to determine underlying differences in virus response.
Keywords: COVID-19; SARS-CoV-2; antiviral therapy; gilteritinib; imatinib; kinase inhibitor; nintedanib.
© 2022 Wiley Periodicals LLC.
Conflict of interest statement
The authors declare no conflict of interest.
Figures




References
Publication types
MeSH terms
Substances
Supplementary concepts
Grants and funding
LinkOut - more resources
Full Text Sources
Medical
Research Materials
Miscellaneous
