

Acceptance of clinical artificial intelligence among physicians and medical students: A systematic review with cross-sectional survey
- PMID: 36117979
- PMCID: PMC9472134
- DOI: 10.3389/fmed.2022.990604
Acceptance of clinical artificial intelligence among physicians and medical students: A systematic review with cross-sectional survey
Abstract
Background: Artificial intelligence (AI) needs to be accepted and understood by physicians and medical students, but few have systematically assessed their attitudes. We investigated clinical AI acceptance among physicians and medical students around the world to provide implementation guidance.
Materials and methods: We conducted a two-stage study, involving a foundational systematic review of physician and medical student acceptance of clinical AI. This enabled us to design a suitable web-based questionnaire which was then distributed among practitioners and trainees around the world.
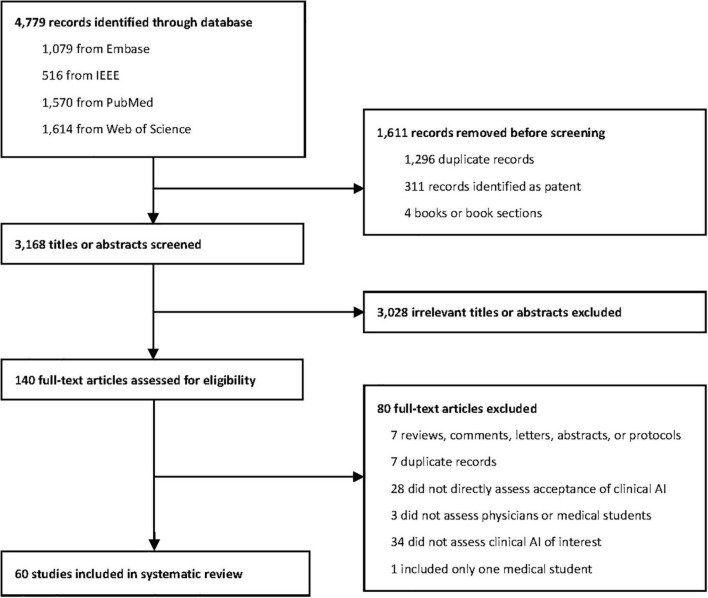
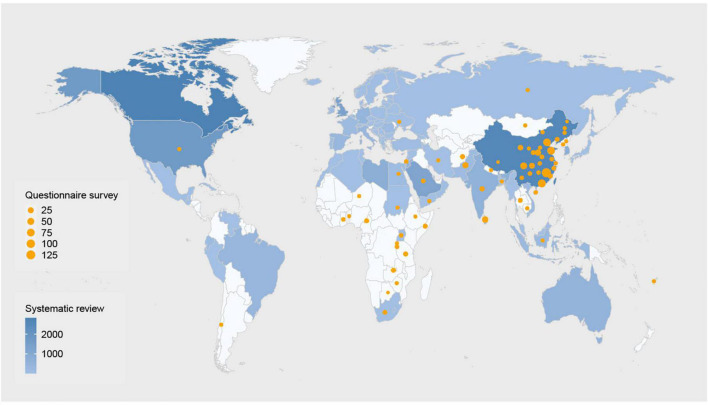
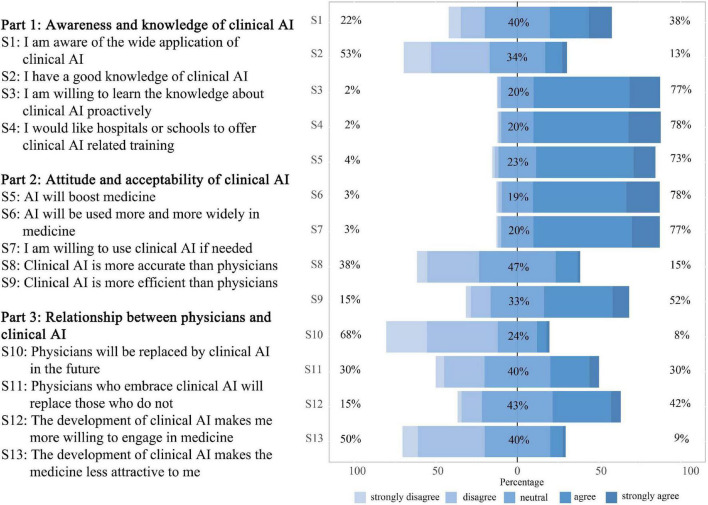
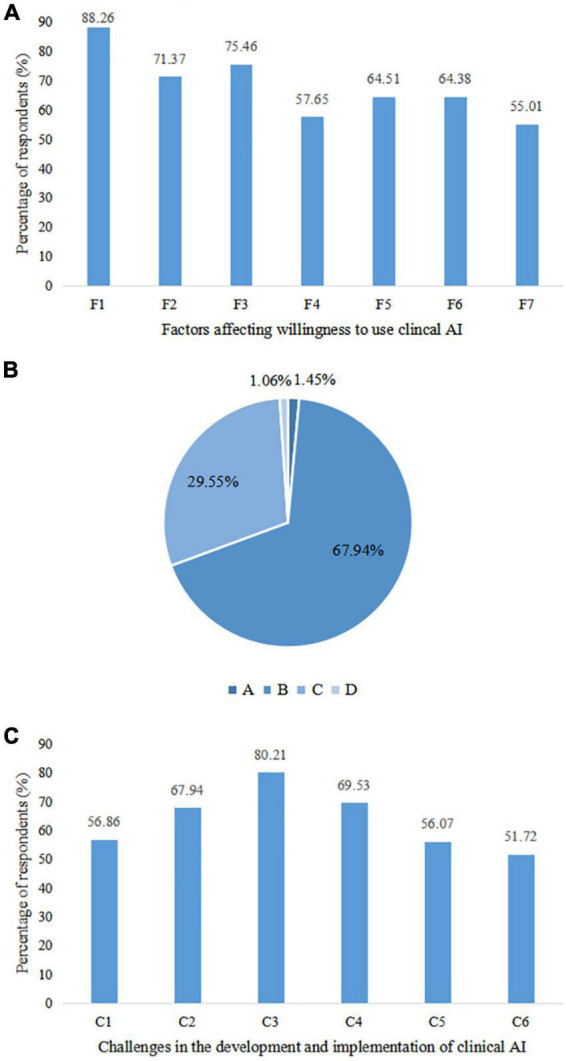
Results: Sixty studies were included in this systematic review, and 758 respondents from 39 countries completed the online questionnaire. Five (62.50%) of eight studies reported 65% or higher awareness regarding the application of clinical AI. Although, only 10-30% had actually used AI and 26 (74.28%) of 35 studies suggested there was a lack of AI knowledge. Our questionnaire uncovered 38% awareness rate and 20% utility rate of clinical AI, although 53% lacked basic knowledge of clinical AI. Forty-five studies mentioned attitudes toward clinical AI, and over 60% from 38 (84.44%) studies were positive about AI, although they were also concerned about the potential for unpredictable, incorrect results. Seventy-seven percent were optimistic about the prospect of clinical AI. The support rate for the statement that AI could replace physicians ranged from 6 to 78% across 40 studies which mentioned this topic. Five studies recommended that efforts should be made to increase collaboration. Our questionnaire showed 68% disagreed that AI would become a surrogate physician, but believed it should assist in clinical decision-making. Participants with different identities, experience and from different countries hold similar but subtly different attitudes.
Conclusion: Most physicians and medical students appear aware of the increasing application of clinical AI, but lack practical experience and related knowledge. Overall, participants have positive but reserved attitudes about AI. In spite of the mixed opinions around clinical AI becoming a surrogate physician, there was a consensus that collaborations between the two should be strengthened. Further education should be conducted to alleviate anxieties associated with change and adopting new technologies.
Keywords: acceptance; artificial intelligence (AI); attitude; medical students; physicians.
Copyright © 2022 Chen, Zhang, Cai, Seery, Gonzalez, Ali, Ren, Qiao, Xue and Jiang.
Conflict of interest statement
The authors declare that the research was conducted in the absence of any commercial or financial relationships that could be construed as a potential conflict of interest.
Figures

References
-
- FDA. Artificial Intelligence and Machine Learning (Ai/Ml)-Enabled Medical Devices. (2021). Available online at: https://www.fda.gov/medical-devices/software-medical-device-samd/artific... (accessed May 13, 2022).
-
- Liu X, Faes L, Kale AU, Wagner SK, Fu DJ, Bruynseels A, et al. A comparison of deep learning performance against health-care professionals in detecting diseases from medical imaging: a systematic review and meta-analysis. Lancet Digit Health. (2019) 1:e271–97. 10.1016/s2589-7500(19)30123-2 - DOI - PubMed
LinkOut - more resources
Full Text Sources