

A scoring system developed from a nomogram to differentiate active pulmonary tuberculosis from inactive pulmonary tuberculosis
- PMID: 36118035
- PMCID: PMC9478038
- DOI: 10.3389/fcimb.2022.947954
A scoring system developed from a nomogram to differentiate active pulmonary tuberculosis from inactive pulmonary tuberculosis
Abstract
Purpose: This study aimed to develop and validate a scoring system based on a nomogram of common clinical metrics to discriminate between active pulmonary tuberculosis (APTB) and inactive pulmonary tuberculosis (IPTB).
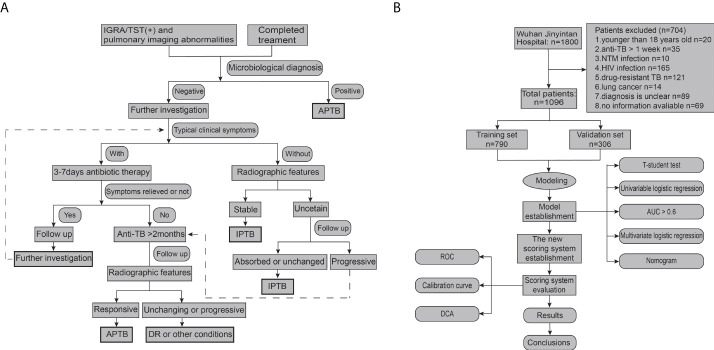
Patients and methods: A total of 1096 patients with pulmonary tuberculosis (PTB) admitted to Wuhan Jinyintan Hospital between January 2017 and December 2019 were included in this study. Of these patients with PTB, 744 were included in the training cohort (70%; 458 patients with APTB, and 286 patients with IPTB), and 352 were included in the validation cohort (30%; 220 patients with APTB, and 132 patients with IPTB). Data from 744 patients from the training cohort were used to establish the diagnostic model. Routine blood examination indices and biochemical indicators were collected to construct a diagnostic model using the nomogram, which was then transformed into a scoring system. Furthermore, data from 352 patients from the validation cohort were used to validate the scoring system.
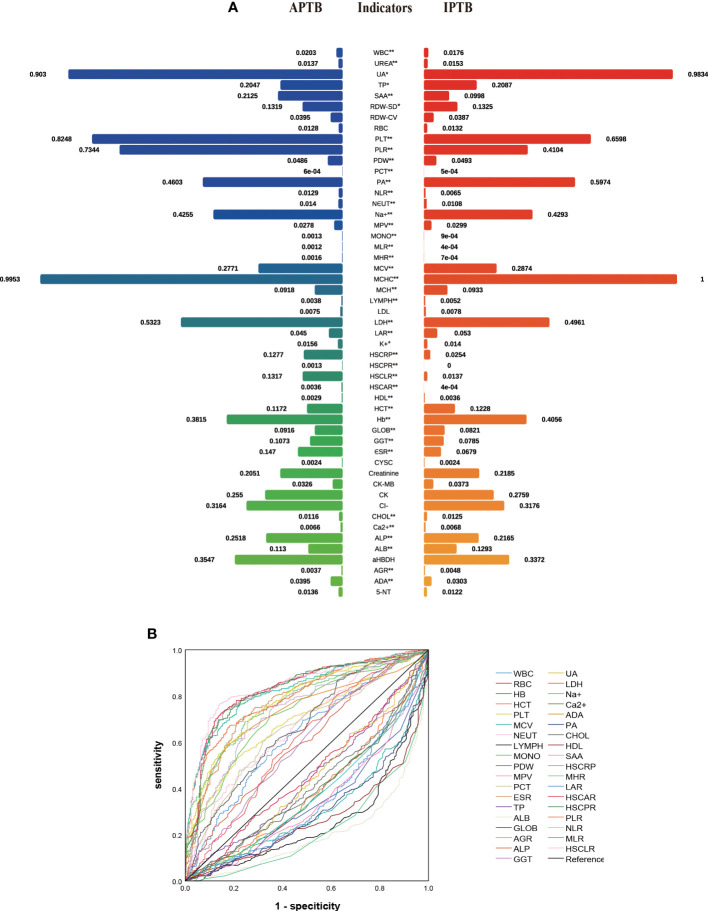
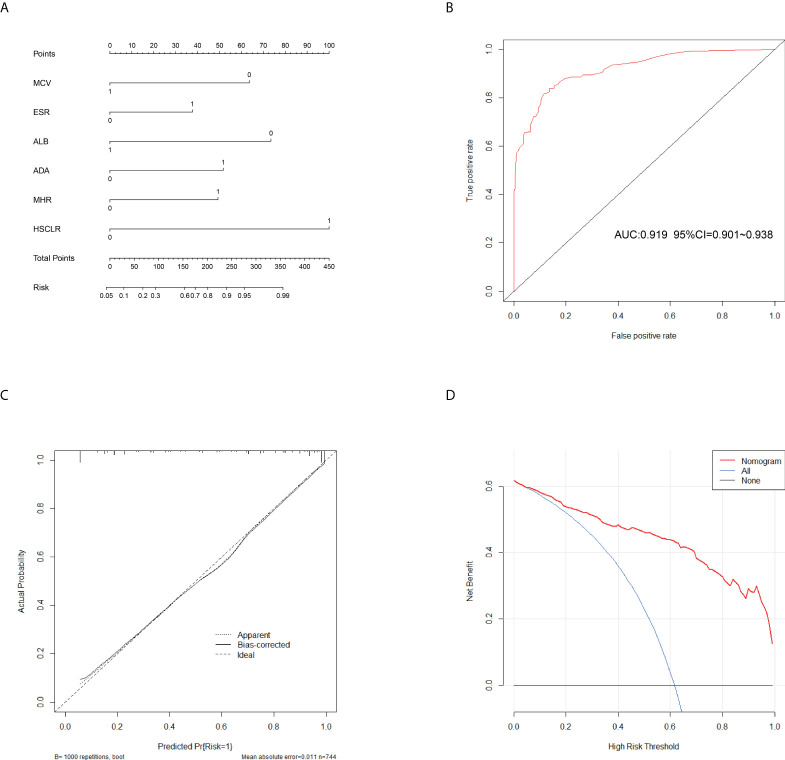
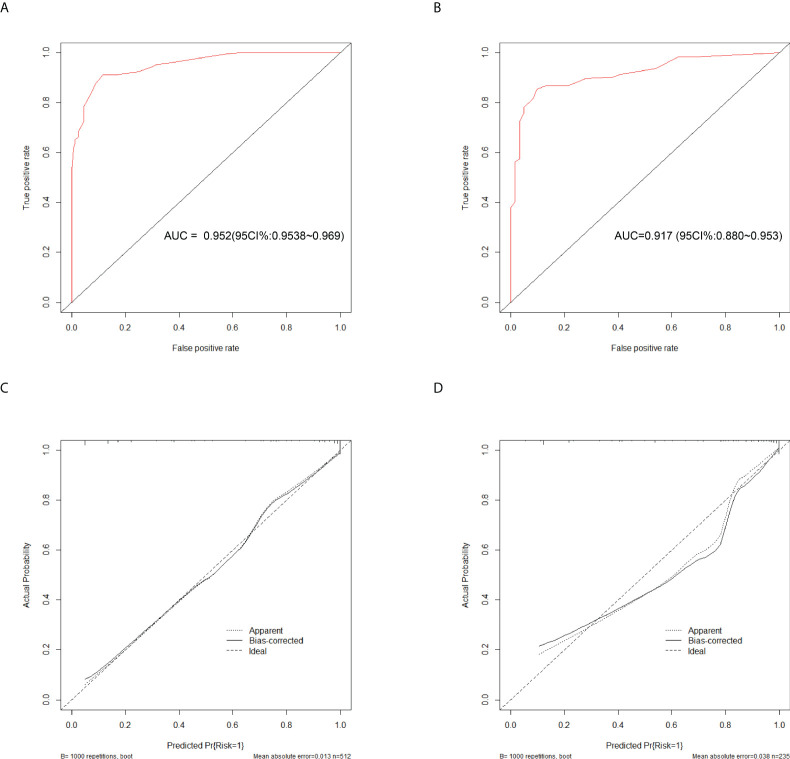
Results: Six variables were selected to construct the prediction model. In the scoring system, the mean corpuscular volume, erythrocyte sedimentation rate, albumin level, adenosine deaminase level, monocyte-to-high-density lipoprotein ratio, and high-sensitivity C-reactive protein-to-lymphocyte ratio were 6, 4, 7, 5, 5, and 10, respectively. When the cut-off value was 15.5, the scoring system for recognizing APTB and IPTB exhibited excellent diagnostic performance. The area under the curve, specificity, and sensitivity of the training cohort were 0.919, 84.06%, and 86.36%, respectively, whereas those of the validation cohort were 0.900, 82.73, and 86.36%, respectively.
Conclusion: This study successfully constructed a scoring system for distinguishing APTB from IPTB that performed well.
Keywords: Active pulmonary tuberculosis; differential diagnosis; inactive pulmonary tuberculosis; nomogram; scoring system.
Copyright © 2022 Yu, Yan, Tian, Weng, Luo, Wei, Long, Ma, Gong and Wang.
Conflict of interest statement
The authors declare that the research was conducted in the absence of any commercial or financial relationships that could be construed as a potential conflict of interest.
Figures
Similar articles
-
Construction and Validation of a Diagnostic Scoring System for Predicting Active Pulmonary Tuberculosis in Patients with Positive T-SPOT Based on Indicators Associated with Coagulation and Inflammation: A Retrospective Cross-Sectional Study.Infect Drug Resist. 2023 Aug 31;16:5755-5764. doi: 10.2147/IDR.S410923. eCollection 2023. Infect Drug Resist. 2023. PMID: 37670979 Free PMC article.
-
Analysis of factors influencing bronchiectasis patients with active pulmonary tuberculosis and development of a nomogram prediction model.Front Med (Lausanne). 2024 Nov 8;11:1457048. doi: 10.3389/fmed.2024.1457048. eCollection 2024. Front Med (Lausanne). 2024. PMID: 39582970 Free PMC article.
-
The Novel Predictive Biomarkers for Type 2 Diabetes Mellitus in Active Pulmonary Tuberculosis Patients.Infect Drug Resist. 2022 Aug 13;15:4529-4539. doi: 10.2147/IDR.S377465. eCollection 2022. Infect Drug Resist. 2022. PMID: 35992755 Free PMC article.
-
The role of 99mTc-MIBI scintigraphy in the management of patients with pulmonary tuberculosis.Eur Rev Med Pharmacol Sci. 2012 May;16(5):622-9. Eur Rev Med Pharmacol Sci. 2012. PMID: 22774403
-
Technetium-99m-tetrofosmin scintigraphy in pulmonary tuberculosis.J Nucl Med. 1998 Dec;39(12):2116-20. J Nucl Med. 1998. PMID: 9867153
Cited by
-
Predictors contributing to the estimation of pulmonary tuberculosis among adults in a resource-limited setting: A systematic review of diagnostic predictions.SAGE Open Med. 2024 May 16;12:20503121241243238. doi: 10.1177/20503121241243238. eCollection 2024. SAGE Open Med. 2024. PMID: 38764538 Free PMC article. Review.
-
18F-fluorodeoxyglucose PET/CT scans for thoracic tuberculosis: current evidence and future perspectives.Eur Respir Rev. 2025 Jun 25;34(176):240289. doi: 10.1183/16000617.0289-2024. Print 2025 May. Eur Respir Rev. 2025. PMID: 40562440 Free PMC article. Review.
-
Construction and Validation of a Diagnostic Scoring System for Predicting Active Pulmonary Tuberculosis in Patients with Positive T-SPOT Based on Indicators Associated with Coagulation and Inflammation: A Retrospective Cross-Sectional Study.Infect Drug Resist. 2023 Aug 31;16:5755-5764. doi: 10.2147/IDR.S410923. eCollection 2023. Infect Drug Resist. 2023. PMID: 37670979 Free PMC article.
-
Association Between Monocyte-to-High-Density Lipoprotein Ratio and Prediabetes: A Cross-Sectional Study in Chinese Population.Diabetes Metab Syndr Obes. 2024 Mar 2;17:1093-1103. doi: 10.2147/DMSO.S451189. eCollection 2024. Diabetes Metab Syndr Obes. 2024. PMID: 38450416 Free PMC article.
-
Construction and Validation of a Nomogram to Identify the Risk of Cavitation in Pulmonary Tuberculosis.Infect Drug Resist. 2024 Jul 5;17:2803-2813. doi: 10.2147/IDR.S459330. eCollection 2024. Infect Drug Resist. 2024. PMID: 38989008 Free PMC article.
References
-
- Baruch Baluku J., Musaazi J., Mulwana R., Bengo D., Sekaggya Wiltshire C., Andia-Biraro I. (2020). Sensitivity and specificity of the mean corpuscular volume and CD4/CD8 ratio in discriminating between rifampicin resistant and rifampicin sensitive tuberculosis. J. Clin. Tuberculosis Other Mycobacterial Dis. 21, 100205. doi: 10.1016/j.jctube.2020.100205 - DOI - PMC - PubMed
-
- Bosco M. J., Hou H., Mao L., Wu X., Ramroop K. D., Lu Y., et al. . (2017). The performance of the TBAg/PHA ratio in the diagnosis of active TB disease in immunocompromised patients. Int. J. Infect. Diseases: IJID: Off. Publ. Int. Soc. Infect. Dis. 59, 55–60. doi: 10.1016/j.ijid.2017.03.025 - DOI - PubMed
-
- Chedid C., Kokhreidze E., Tukvadze N., Banu S., Uddin M. K. M., Biswas S., et al. . (2020). Association of baseline white blood cell counts with tuberculosis treatment outcome: a prospective multicentered cohort study. Int. J. Infect. Dis. IJID Off. Publ. Int. Soc. For Infect. Dis. 100, 199–206. doi: 10.1016/j.ijid.2020.09.017 - DOI - PubMed
Publication types
MeSH terms
Substances
LinkOut - more resources
Full Text Sources
Medical
Research Materials