

Refractory ventricular tachycardia treated by a second session of stereotactic arrhythmia radioablation
- PMID: 36118122
- PMCID: PMC9478870
- DOI: 10.1016/j.ctro.2022.07.005
Refractory ventricular tachycardia treated by a second session of stereotactic arrhythmia radioablation
Abstract
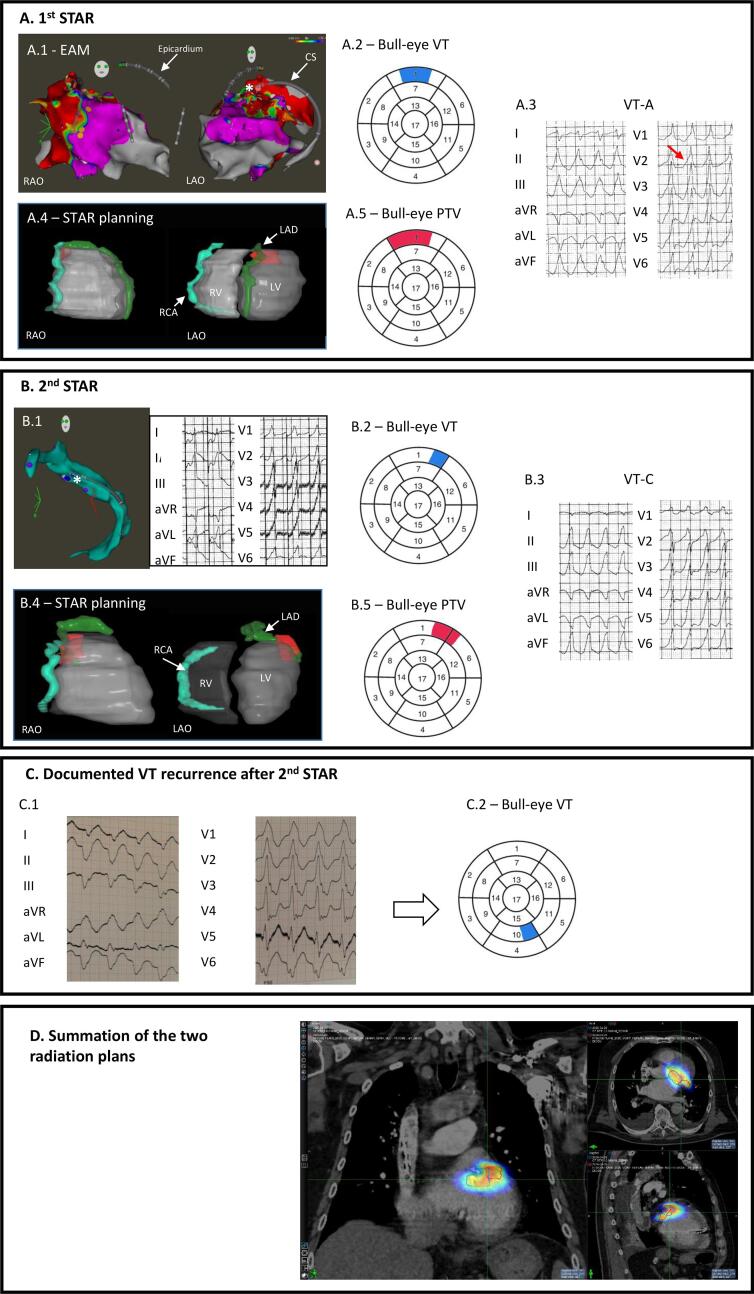
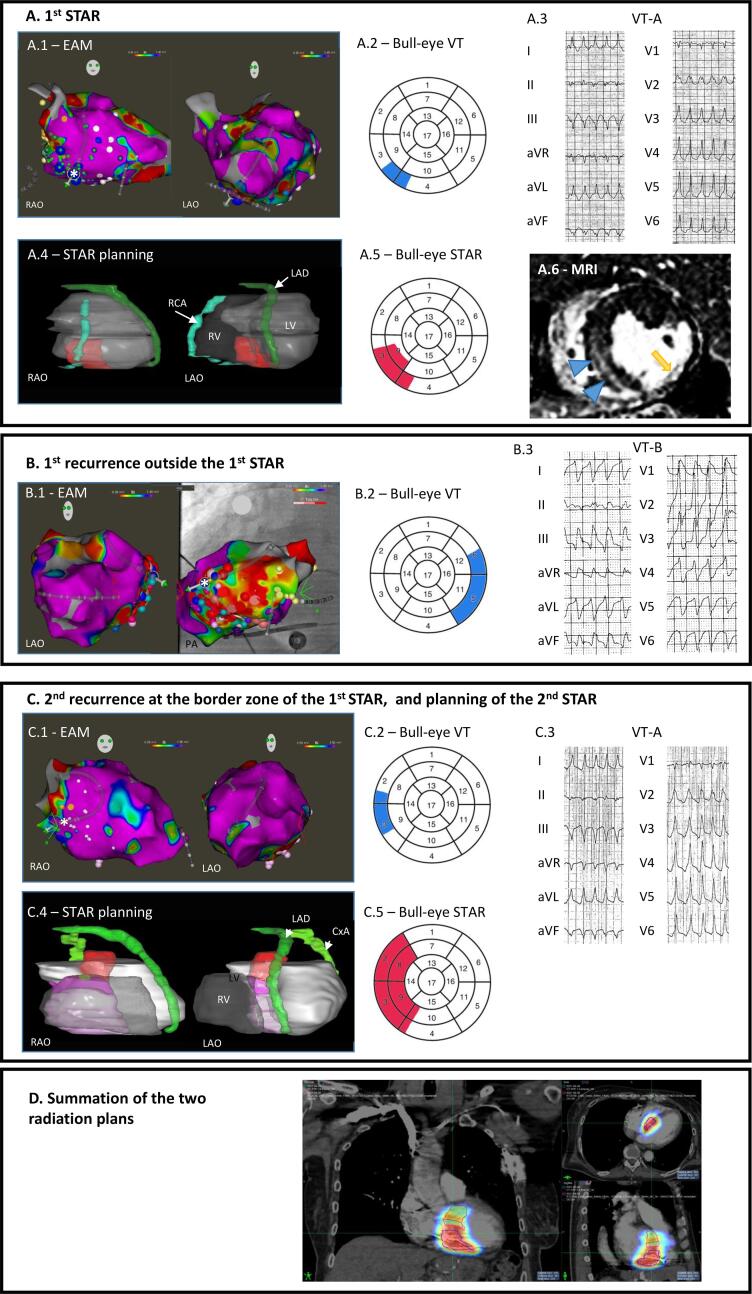
Purpose: Stereotactic arrhythmia radioablation (STAR) is an effective treatment for refractory ventricular tachycardia (VT), but recurrences after STAR were recently published. Herein, we report two cases of successful re-irradiation of the arrhythmogenic substrate.
Cases: We present two cases of re-irradiation after recurrence of a previously treated VT with radioablation at a dose of 20 Gy. The VT exit was localized on the border zone of the irradiated volume, which responded positively to re-irradiation at follow-up.
Conclusion: These two cases show the technical feasibility of re-irradiation to control recurrent VT after a first STAR.
Keywords: Ischemic heart disease; Non-ischemic cardiomyopathy; Stereotactic arrhythmia radioablation (STAR); ventricular tachycardia (VT).
© 2022 Published by Elsevier B.V. on behalf of European Society for Radiotherapy and Oncology.
Conflict of interest statement
The authors declare that they have no known competing financial interests or personal relationships that could have appeared to influence the work reported in this paper.
Figures
References
-
- Neuwirth R., Cvek J., Knybel L., Jiravsky O., Molenda L., Kodaj M., et al. Stereotactic radiosurgery for ablation of ventricular tachycardia. Europace. 2019;21:1088–1095. - PubMed
-
- Lloyd M.S., Wight J., Schneider F., Hoskins M., Attia T., Escott C., et al. Clinical experience of stereotactic body radiation for refractory ventricular tachycardia in advanced heart failure patients. Heart Rhythm. 2020;17(3):415–422. - PubMed
-
- Gianni C., Rivera D., Burkhardt J.D., Pollard B., Gardner E., Maguire P., et al. Stereotactic arrhythmia radioablation for refractory scar-related ventricular tachycardia. Heart Rhythm. 2020;17(8):1241–1248. - PubMed
-
- Jumeau R., Ozsahin M., Schwitter J., Vallet V., Duclos F., Zeverino M., et al. Rescue procedure for an electrical storm using robotic non-invasive cardiac radio-ablation. Radiother Oncol. 2018;128(2):189–191. - PubMed
Publication types
LinkOut - more resources
Full Text Sources
