

Partial Sternal Resections in Primary and Metastatic Tumors with Nonrigid Reconstruction of Chest Wall
- PMID: 36118389
- PMCID: PMC9478070
- DOI: 10.1007/s13193-017-0632-7
Partial Sternal Resections in Primary and Metastatic Tumors with Nonrigid Reconstruction of Chest Wall
Abstract
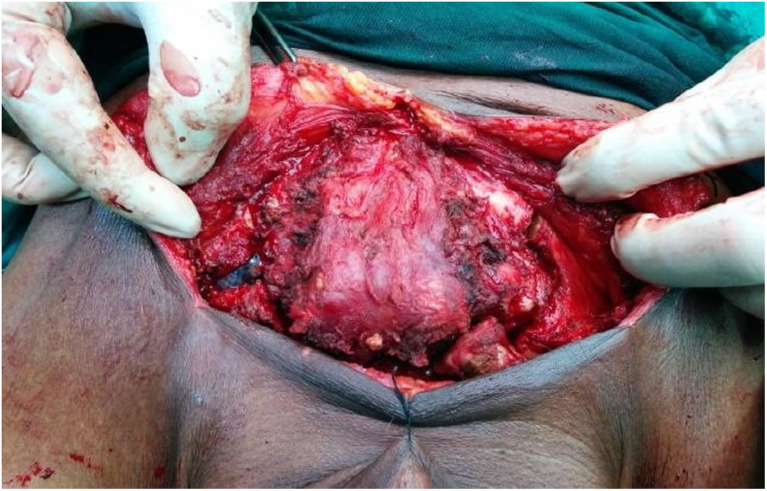
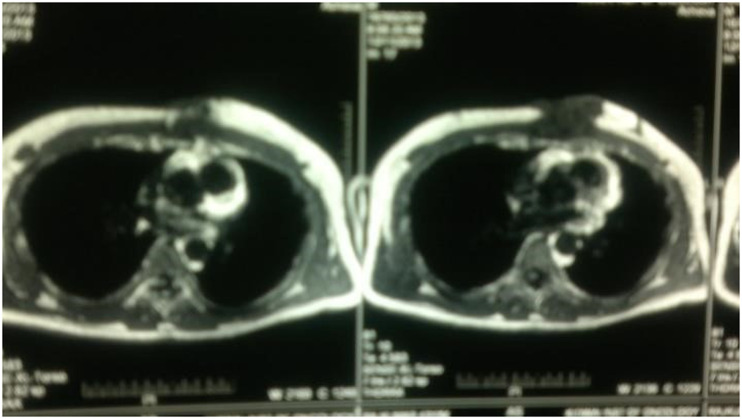
Primary sternal tumors are rare and are often metastatic from neoplasms of lung, breast, thyroid, and kidney. A radical resection is indicated for their management. In recent years many rigid reconstructions are described to prevent pulmonary complications and for protection of intra -thoracic organs. It is known that chest wall is a stable yet flexible structure and hence the optimal functional outcome in spite of rigid reconstructions remains an ongoing challenge. We hypothesized that partial sternal resections does not need a rigid reconstruction and studied the functional outcome in series of five cases where simple reconstructions are done.We did standard excision of sternum and ribs depending on the site. Immediate reconstruction was done using available myocutaneous flaps (TRAM flap, Pectoralis major muscle flap and polypropylene mesh). All cases had smooth postoperative course, had excellent coverage, chest wall stability and minimal donor site morbidity. All had a short hospital stay period (8-12 days) with good functional outcome. We do hereby propose nonrigid reconstruction for partial sternal defects as a good and safe alternative.
Keywords: Neoplasms; Resection; Tumor.
© Indian Association of Surgical Oncology 2017.
Conflict of interest statement
Conflict of InterestThe authors declare that they have no conflict of interest.
Figures





















References
-
- Kluiber R, Bines S, Bradley C, Faber LP, Witt TR. Major chest wall resection for recurrent breast carcinoma. Am Surg. 1991;57:523–530. - PubMed
LinkOut - more resources
Full Text Sources