

Risk of severe COVID-19 outcomes associated with rheumatoid arthritis and phenotypic subgroups: a retrospective, comparative, multicentre cohort study
- PMID: 36118532
- PMCID: PMC9472567
- DOI: 10.1016/S2665-9913(22)00227-2
Risk of severe COVID-19 outcomes associated with rheumatoid arthritis and phenotypic subgroups: a retrospective, comparative, multicentre cohort study
Abstract
Background: Rheumatoid arthritis has been associated with severe COVID-19, but few studies have investigated how phenotypes of rheumatoid arthritis affect these associations. We aimed to investigate the associations between rheumatoid arthritis and phenotypes of interstitial lung disease, serostatus, and bone erosions with COVID-19 severity.
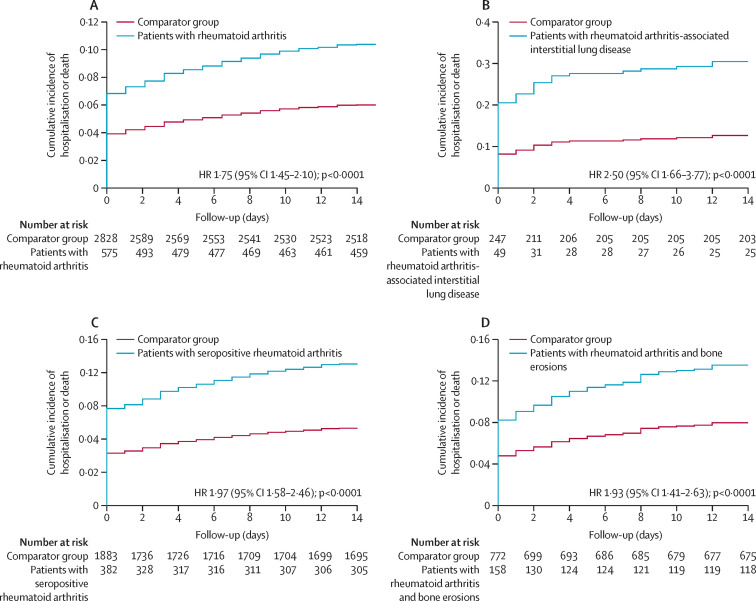
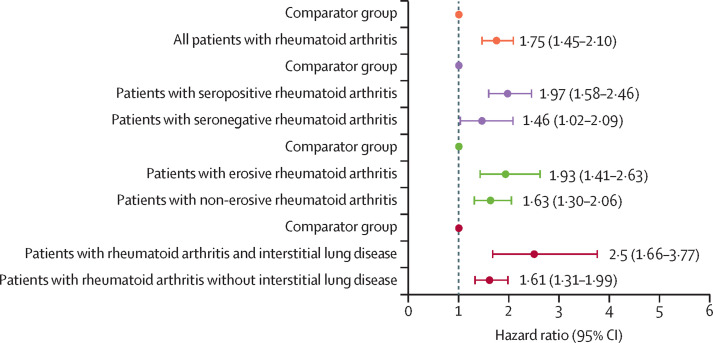
Methods: We did a retrospective, comparative, multicentre cohort study at two large health-care systems (Mayo Clinic [19 hospitals and affiliated outpatient centres] and Mass General Brigham [14 hospitals and affiliated outpatient centres]) in the USA. Consecutive patients with rheumatoid arthritis meeting the 2010 American College of Rheumatology/European League Against Rheumatism classification criteria and who had COVID-19 between March 1, 2020, and June 6, 2021, were matched 1:5 on age, sex, and calendar date with patients without rheumatoid arthritis (comparators). Data were received from electronic health records from Mayo Clinic and Mass General Brigham. We examined subgroups of patients with rheumatoid arthritis by phenotypic features: rheumatoid arthritis-associated interstitial lung disease, seropositivity (for anti-cyclic citrullinated peptide, rheumatoid factor, or both), and bone erosions. Severe COVID-19 was a composite of hospitalisation or death. We used Cox regression to estimate hazard ratios (HR) for severe COVID-19, comparing rheumatoid arthritis and subgroups to the comparator group.
Findings: We identified 582 patients with rheumatoid arthritis and 2875 matched comparators, all of whom had COVID-19 within the study dates. The mean age of those with rheumatoid arthritis was 62 [SD 14] years, 421 (72%) of 582 were women and 161 (28%) were men, 457 (79%) were White, 65 (11%) were Hispanic or Latino, and 41 (7%) were Black. Among patients with rheumatoid arthritis, 50 (9%) of 582 had interstitial lung disease, 388 (68%) of 568 were seropositive, and 159 (27%) of 582 had bone erosions. Severe COVID-19 occurred in 126 (22%) of 582 patients with rheumatoid arthritis versus 363 (13%) 2875 in the comparator group. Patients with rheumatoid arthritis had an HR of 1·75 (95% CI 1·45-2·10) for severe COVID-19 versus the comparator group. Patients with rheumatoid arthritis-associated interstitial lung disease had an HR of 2·50 (1·66-3·77) versus the comparator group for severe COVID-19. The risk for severe COVID-19 was also higher in patients with rheumatoid arthritis who were seropositive (HR 1·97 [95% CI 1·58-2·46]) or had erosive disease (1·93 [1·41-2·63]) than for those in the comparator group.
Interpretation: Patients with rheumatoid arthritis have an increased risk of severe COVID-19 across phenotypic subgroups, especially among patients with interstitial lung disease. These findings suggest that rheumatoid arthritis with interstitial lung disease, or its treatment, might be a substantial contributor to severe COVID-19 outcomes for patients with rheumatoid arthritis.
Funding: None.
© 2022 Elsevier Ltd. All rights reserved.
Conflict of interest statement
NJP reports consulting fees from FVC Health, unrelated to this work; and is supported by the US National Institutes of Health Ruth L Kirschstein Institutional National Research Service Award (T32-AR-007258). JAS has received research support from Bristol Myers Squibb; consulted for AbbVie, Amgen, Boehringer Ingelheim, Bristol Myers Squibb, Gilead, Inova Diagnostics, Janssen, Optum, and Pfizer, unrelated to this work; and is supported by the US National Institute of Arthritis and Musculoskeletal and Skin Diseases (R01 AR077607, P30 AR070253, and P30 AR072577) and the R Bruce and Joan M Mickey Research Scholar Fund. ZSW reports research support from Bristol-Myers Squibb and Principia/Sanofi; consulting fees from Viela Bio, Horizon, Zenas Biopharma, Shionogi, Sanofi, and MedPace, unrelated to this work; and is supported by the US National Institute of Arthritis and Musculoskeletal and Skin Diseases (K23AR073334 and R03AR078938), the Rheumatology Research Foundation, and Massachusetts General Hospital Department of Medicine. AD-G has received unrelated grant funding from the US Centers for Disease Control and Prevention, the Rheumatology Research Foundation Career Development Award, and the Robert D and Patricia E Kern Center for the Science of Health Care Delivery. All other authors have no competing interests. The content is solely the responsibility of the authors and does not necessarily represent the official views of Harvard University, its affiliated academic health-care centres, or the US National Institutes of Health.
Figures
Similar articles
-
Mortality and immune-related adverse events after immune checkpoint inhibitor initiation for cancer among patients with pre-existing rheumatoid arthritis: a retrospective, comparative, cohort study.Lancet Rheumatol. 2023 May;5(5):e274-e283. doi: 10.1016/s2665-9913(23)00064-4. Epub 2023 Mar 27. Lancet Rheumatol. 2023. PMID: 37841635 Free PMC article.
-
Rheumatoid Arthritis Disease Activity Predicting Incident Clinically Apparent Rheumatoid Arthritis-Associated Interstitial Lung Disease: A Prospective Cohort Study.Arthritis Rheumatol. 2019 Sep;71(9):1472-1482. doi: 10.1002/art.40904. Epub 2019 Aug 4. Arthritis Rheumatol. 2019. PMID: 30951251 Free PMC article.
-
Safety, tolerability, and efficacy of pirfenidone in patients with rheumatoid arthritis-associated interstitial lung disease: a randomised, double-blind, placebo-controlled, phase 2 study.Lancet Respir Med. 2023 Jan;11(1):87-96. doi: 10.1016/S2213-2600(22)00260-0. Epub 2022 Sep 5. Lancet Respir Med. 2023. PMID: 36075242 Clinical Trial.
-
Rheumatoid Arthritis-Associated Interstitial Lung Disease and Idiopathic Pulmonary Fibrosis: Shared Mechanistic and Phenotypic Traits Suggest Overlapping Disease Mechanisms.Rev Invest Clin. 2015 Sep-Oct;67(5):280-6. Rev Invest Clin. 2015. PMID: 26696331 Free PMC article. Review.
-
Tofacitinib for Treating Rheumatoid Arthritis After the Failure of Disease-Modifying Anti-rheumatic Drugs: An Evidence Review Group Perspective of a NICE Single Technology Appraisal.Pharmacoeconomics. 2018 Sep;36(9):1063-1072. doi: 10.1007/s40273-018-0639-0. Pharmacoeconomics. 2018. PMID: 29546668 Review.
Cited by
-
Hospitalization, Critical Illness, and Mortality Outcomes of COVID-19 in Patients With Rheumatoid Arthritis.ACR Open Rheumatol. 2023 Sep;5(9):465-473. doi: 10.1002/acr2.11580. Epub 2023 Aug 2. ACR Open Rheumatol. 2023. PMID: 37530460 Free PMC article.
-
Exploring the Linkages Among Chronic Illness, Substance Use, and COVID-19 Infection in Adults Aged 50 Years and Older: Retrospective Cross-Sectional Analysis of National Representative Data.JMIR Aging. 2024 Oct 15;7:e63024. doi: 10.2196/63024. JMIR Aging. 2024. PMID: 39405517 Free PMC article.
-
Beneficial effect of temporary methotrexate interruption on B and T cell responses upon SARS-CoV-2 vaccination in patients with rheumatoid arthritis or psoriatic arthritis.NPJ Vaccines. 2024 Jan 30;9(1):21. doi: 10.1038/s41541-024-00805-3. NPJ Vaccines. 2024. PMID: 38291047 Free PMC article.
-
Association between pre-existing chronic conditions and severity of first SARS-CoV-2 infection symptoms among adults living in Canada: a population-based survey analysis from January 2020 to August 2022.BMC Public Health. 2025 Mar 12;25(1):981. doi: 10.1186/s12889-025-22041-7. BMC Public Health. 2025. PMID: 40075342 Free PMC article.
-
Patients with systemic autoimmune rheumatic diseases remain at risk for hospitalisation for COVID-19 infection in the Omicron era (2022-2024): a retrospective cohort study.RMD Open. 2025 Mar 5;11(1):e005114. doi: 10.1136/rmdopen-2024-005114. RMD Open. 2025. PMID: 40044572 Free PMC article.
References
-
- Figueroa-Parra G, Aguirre-Garcia GM, Gamboa-Alonso CM, Camacho-Ortiz A, Galarza-Delgado DA. Are my patients with rheumatic diseases at higher risk of COVID-19? Ann Rheum Dis. 2020;79:839–840. - PubMed
-
- Pablos JL, Galindo M, Carmona L, et al. Clinical outcomes of hospitalised patients with COVID-19 and chronic inflammatory and autoimmune rheumatic diseases: a multicentric matched cohort study. Ann Rheum Dis. 2020;79:1544–1549. - PubMed
Grants and funding
LinkOut - more resources
Full Text Sources
