

Thyroid cancer harboring PTEN and TP53 mutations: A peculiar molecular and clinical case report
- PMID: 36119511
- PMCID: PMC9478947
- DOI: 10.3389/fonc.2022.949098
Thyroid cancer harboring PTEN and TP53 mutations: A peculiar molecular and clinical case report
Abstract
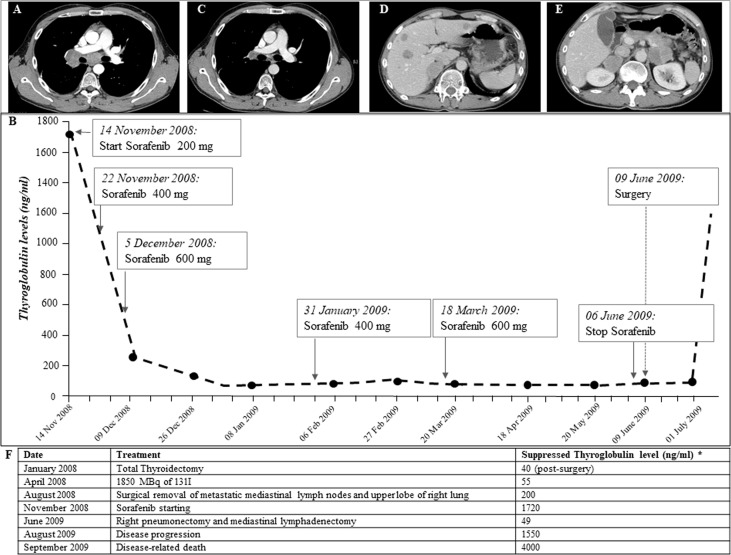
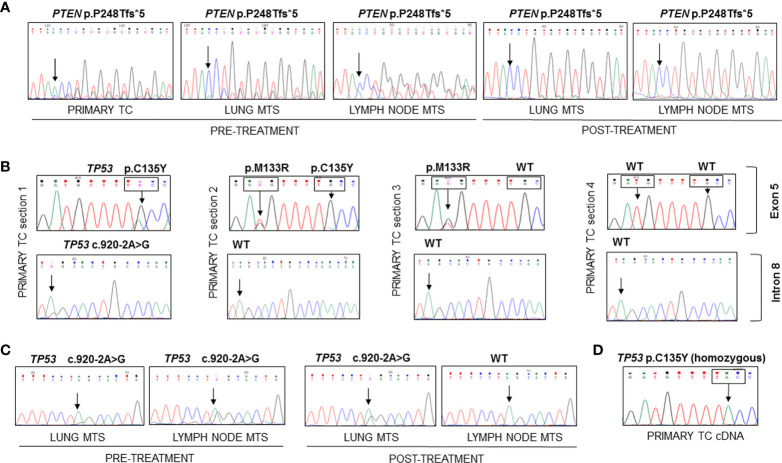
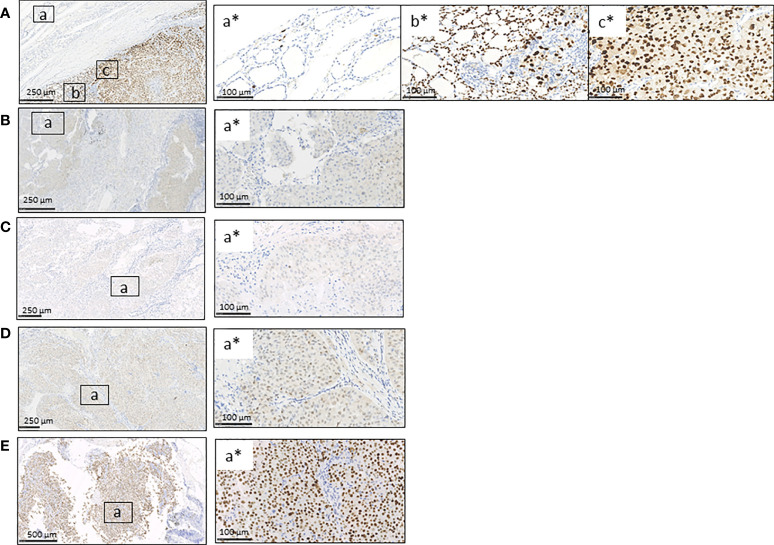
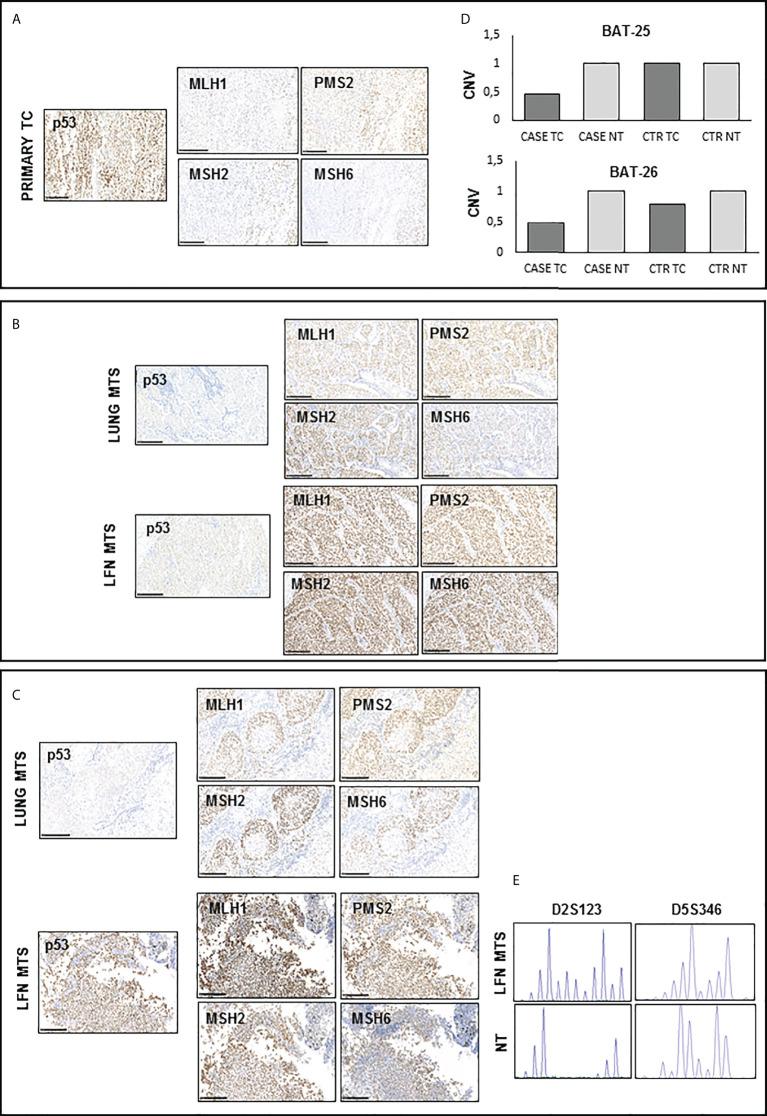
To date, the molecular mechanisms that underline aggressiveness and resistance to tyrosine kinase inhibitors in some thyroid carcinomas (TCs) are not known yet. We report the case of a young patient with a metastatic poorly differentiated (PDTC) and follicular thyroid carcinoma (FTC) refractory to conventional therapies and to Sorafenib. The patient, despite an initial partial response, died of progressive disease 21 months after diagnosis. The genetic analysis performed on the primary tumor and on lymph nodes and distant metastases allowed to identify a frameshift mutation (p.P248Tfs*5) in the PTEN gene, never described in TC. This mutation was present in the primary tumor and, with a lower allelic frequency, in metastases diagnosed after treatment with Sorafenib. Mutations in TP53 (p.C135Y and c.920-2A>G previously detected in anaplastic carcinomas and p.M133R never found in TC) were also detected in the primary tissue together with a mono-allelic expression of the p.C135Y mutant at RNA level. At metastatic sites level, we found only the TP53 splicing mutation c.920-2A>G. The presence of defects in mismatch repair (MMR) proteins and genomic instability was also evaluated. The primary tumor showed a partial expression of MMR proteins together with a strong genomic instability. In conclusion, we demonstrated that the rare combination of somatic PTEN and TP53 mutations in a patient with a metastatic FTC, together with the presence of tumor heterogeneity and genomic instability, might be associated with a high tumor aggressiveness and resistance to treatments.
Keywords: PTEN; Sorafenib; TP53; aggressive follicular thyroid cancer; microsatellite instability; mismatch repair proteins; tyrosine kinase inhibitor.
Copyright © 2022 Colombo, Pogliaghi, Tosi, Muzza, Bulfamante, Persani, Fugazzola and Cirello.
Conflict of interest statement
The authors declare that the research was conducted in the absence of any commercial or financial relationships that could be construed as a potential conflict of interest.
Figures
References
Publication types
LinkOut - more resources
Full Text Sources
Research Materials
Miscellaneous