

Clinical feasibility and treatment outcomes with nonselected autologous tumor-infiltrating lymphocyte therapy in patients with advanced cutaneous melanoma
- PMID: 36119832
- PMCID: PMC9441996
Clinical feasibility and treatment outcomes with nonselected autologous tumor-infiltrating lymphocyte therapy in patients with advanced cutaneous melanoma
Abstract
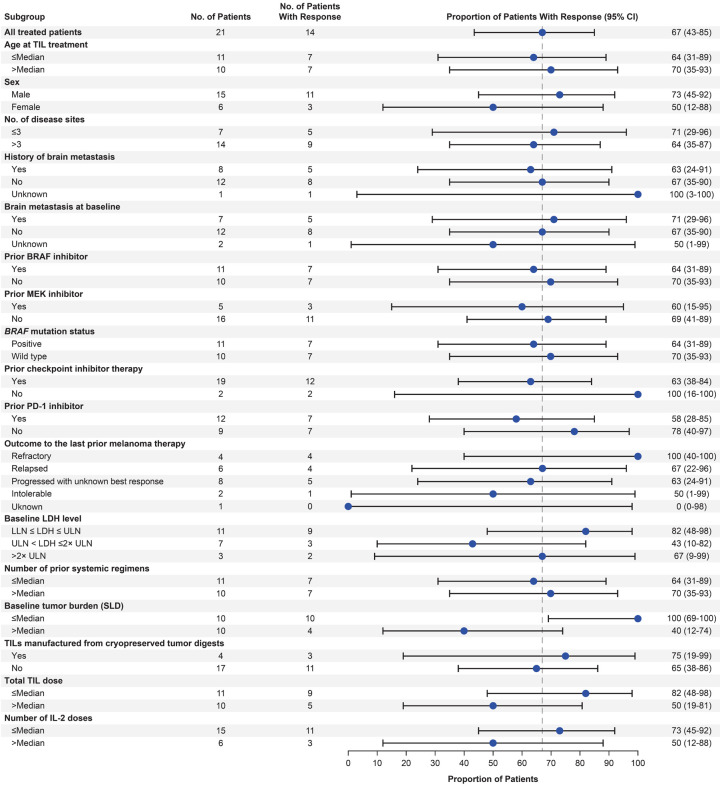
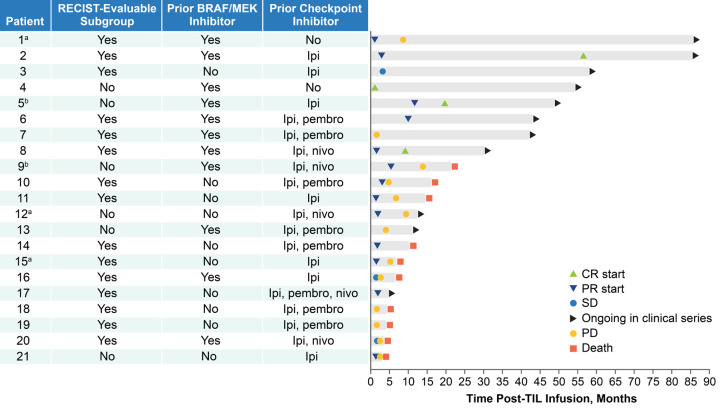
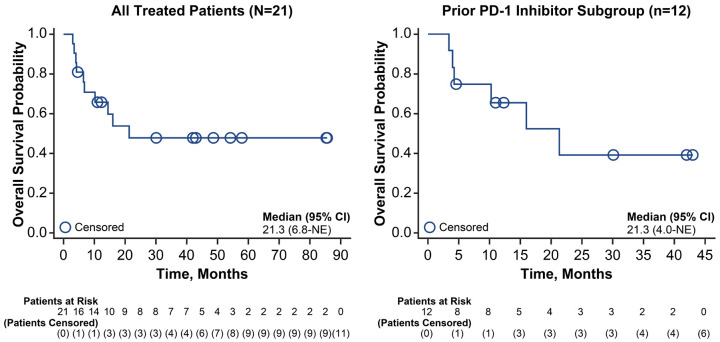
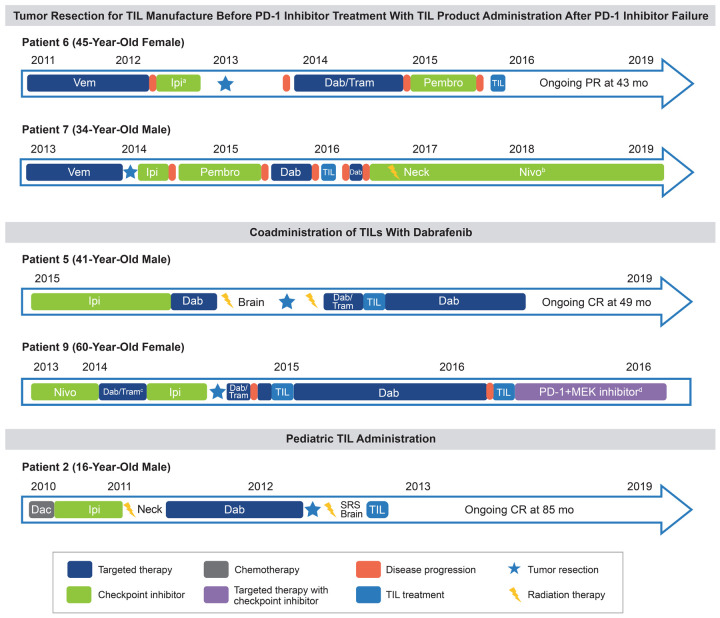
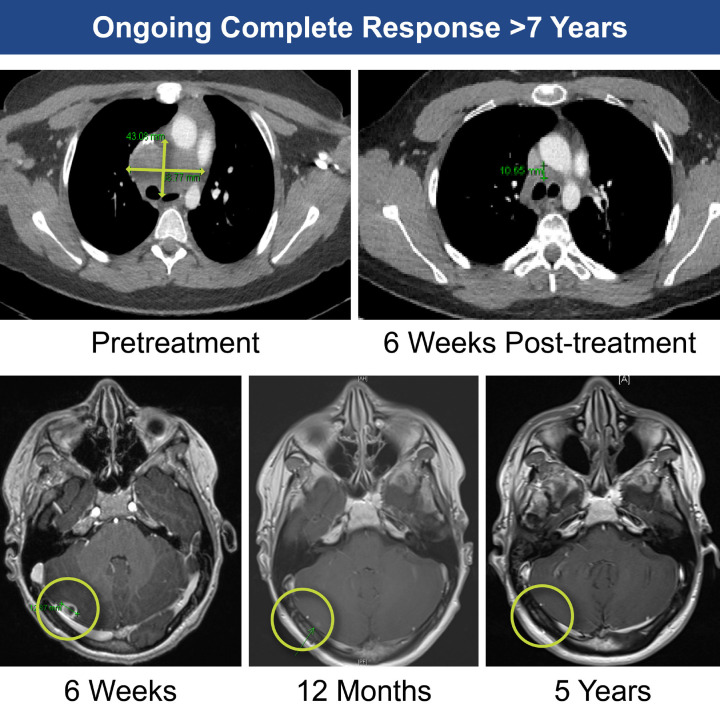
Nonselected autologous tumor-infiltrating lymphocytes (TILs) may provide advantages over other treatments for solid tumors, including checkpoint inhibitor-refractory melanoma. This retrospective analysis reports a single-center experience of nonselected autologous TILs derived from digested tumors for compassionate use treatment of advanced cutaneous melanoma, including after programmed cell death protein 1 (PD-1) inhibition. Patients with histologically confirmed metastatic cutaneous melanoma and no standard-of-care treatment options underwent tumor resection for TIL product manufacturing. Patients received lymphodepleting chemotherapy with cyclophosphamide for 2 days and fludarabine for 5 days, followed by a single TIL infusion and post-TIL high-dose interleukin (IL)-2. Safety assessments included clinically significant adverse events (AEs). Efficacy assessments included overall response rate (ORR), complete response (CR) rate, disease control rate (DCR), and overall survival. Between October 2011 and August 2019, 21 patients underwent treatment (median follow-up time, 52.2 months from TIL infusion). Among all treated patients, median age was 45 years, median number of disease sites was 4, 100% had M1c or M1d disease, and 90% received prior checkpoint inhibitor. Twelve patients received TILs after prior PD-1 inhibition. The safety profile among all treated patients and the prior PD-1 inhibitor subgroup was generally consistent with lymphodepletion and high-dose IL-2. No treatment-related deaths occurred. Among all patients, the ORR was 67%, CR rate was 19%, and the DCR was 86%, which was consistent with that observed in the prior PD-1 inhibitor subgroup (58%, 8%, and 75%, respectively). Median overall survival in all treated patients and the prior PD-1 inhibitor subgroup was 21.3 months. In total, 5 patients (24%) had durable ongoing responses (>30 months post-TIL infusion) at data cutoff, and all patients who achieved CR remained alive and disease free. To further illustrate how TIL therapy may integrate into established treatment paradigms, several case studies of patients treated in this series were included. Overall, these data demonstrate that manufacturing of nonselected autologous TILs from tumor digests is feasible and resulted in high rates of durable response in poor-risk patient populations, which may address significant unmet medical need.
Keywords: PD-1 inhibitor; T cell; Tumor-infiltrating lymphocytes; checkpoint inhibition; compassionate use; immunology; immunotherapy; interleukin-2; melanoma.
AJCR Copyright © 2022.
Conflict of interest statement
M. Pillai reports speakers’ bureau participation for Bristol Myers Squibb, Ipsen, Pfizer, and Novartis; and travel support from EUSA Pharma and Bristol Myers Squibb. Y. Jiang, P. Velazquez, D. Chonzi, and Z. J. Roberts report employment with and stock or other ownership in Instil Bio, Inc. P. C. Lorigan reports honoraria from Amgen, Merck, Merck Sharp & Dohme (MSD), NeraCare GmbH, Novartis, Oncology Education, Pierre Fabre, and Roche; consultancy or advisory role for Amgen, Bristol Myers Squibb, MSD, Nektar, Novartis, and Pierre Fabre; speakers’ bureau participation for Bristol Myers Squibb, MSD, Novartis, and Pierre Fabre; research funding from Bristol Myers Squibb; and travel support from Bristol Myers Squibb and MSD. F. C. Thistlethwaite reports consulting or advisory role for Achilles, Bayer, Bristol Myers Squibb, Evelo Therapeutics, GSK, T-knife, and Zelluna Immunotherapy; research funding from Novartis; and serves as the coordinating or local physician investigator for AbbVie, Achilles Ltd, Adaptimmune, Agalimmune, AstraZeneca, AVEO, Bristol Myers Squibb, Chugai Pharmaceutical Co., CytomX, Daiichi Sankyo, GenMab, GSK, Immunocore, Incyte, Janssen, Kymab Ltd, Millennium Pharmaceuticals/Takeda, Novartis, Pfizer, Roche, and Synthon. M. Thomas reports employment with Cellular Therapeutics, Ltd, Immetacyte, Ltd, and Instil Bio, Inc. N. Kirillova reports former employment with and stock or other ownership in Immetacyte, Inc; and stock or other ownership in Instil Bio, Inc. J. S. Bridgeman reports employment with Instil Bio, Inc; stock or other ownership in Immetacyte and Instil Bio, Inc; and patents, royalties, or other intellectual property from Instil Bio, Inc. G. Kueberuwa reports employment with, stock or other ownership in, and patents, royalties or other intellectual property from Instil Bio, Inc. S. Biswas reports employment with Instil Bio, Inc; stock or other ownership in Instil Bio, Inc. and Kite, a Gilead Company; and patents, royalties, or other intellectual property from City of Hope. R. D. Guest reports employment with, stock or other ownership in, and patents, royalties, or other intellectual property from Instil Bio, Inc; and leadership role at Immetacyte, Inc. R. E. Hawkins reports employment with and stock or other ownership in Instil Bio, Inc; consultancy or advisory role for Anaveon AG and NovalGen, Ltd; and nonexecutive director for and stock or other ownership in Bivictrix Plc.
Figures
References
-
- Hamid O, Robert C, Daud A, Hodi FS, Hwu WJ, Kefford R, Wolchok JD, Hersey P, Joseph RW, Weber JS, Dronca R, Gangadhar TC, Patnaik A, Zarour H, Joshua AM, Gergich K, Elassaiss-Schaap J, Algazi A, Mateus C, Boasberg P, Tumeh PC, Chmielowski B, Ebbinghaus SW, Li XN, Kang SP, Ribas A. Safety and tumor responses with lambrolizumab (anti-PD-1) in melanoma. N Engl J Med. 2013;369:134–144. - PMC - PubMed
-
- Hodi FS, O’Day SJ, McDermott DF, Weber RW, Sosman JA, Haanen JB, Gonzalez R, Robert C, Schadendorf D, Hassel JC, Akerley W, van den Eertwegh AJ, Lutzky J, Lorigan P, Vaubel JM, Linette GP, Hogg D, Ottensmeier CH, Lebbé C, Peschel C, Quirt I, Clark JI, Wolchok JD, Weber JS, Tian J, Yellin MJ, Nichol GM, Hoos A, Urba WJ. Improved survival with ipilimumab in patients with metastatic melanoma. N Engl J Med. 2010;363:711–723. - PMC - PubMed
-
- Topalian SL, Hodi FS, Brahmer JR, Gettinger SN, Smith DC, McDermott DF, Powderly JD, Carvajal RD, Sosman JA, Atkins MB, Leming PD, Spigel DR, Antonia SJ, Horn L, Drake CG, Pardoll DM, Chen L, Sharfman WH, Anders RA, Taube JM, McMiller TL, Xu H, Korman AJ, Jure-Kunkel M, Agrawal S, McDonald D, Kollia GD, Gupta A, Wigginton JM, Sznol M. Safety, activity, and immune correlates of anti-PD-1 antibody in cancer. N Engl J Med. 2012;366:2443–2454. - PMC - PubMed
-
- Flaherty KT, Infante JR, Daud A, Gonzalez R, Kefford RF, Sosman J, Hamid O, Schuchter L, Cebon J, Ibrahim N, Kudchadkar R, Burris HA 3rd, Falchook G, Algazi A, Lewis K, Long GV, Puzanov I, Lebowitz P, Singh A, Little S, Sun P, Allred A, Ouellet D, Kim KB, Patel K, Weber J. Combined BRAF and MEK inhibition in melanoma with BRAF V600 mutations. N Engl J Med. 2012;367:1694–1703. - PMC - PubMed
LinkOut - more resources
Full Text Sources
Other Literature Sources
Research Materials