

Increased Rates of Supplement-Associated Oxalate Nephropathy During COVID-19 Pandemic
- PMID: 36120391
- PMCID: PMC9464307
- DOI: 10.1016/j.ekir.2022.09.002
Increased Rates of Supplement-Associated Oxalate Nephropathy During COVID-19 Pandemic
Abstract
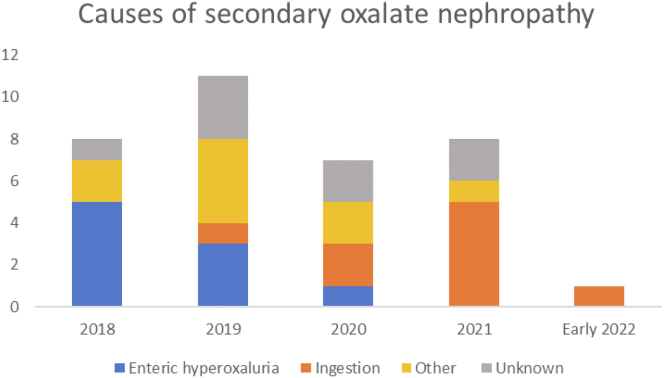
Introduction: Causes of secondary oxalate nephropathy include enteric dysfunction and excessive intake of oxalate or oxalate precursors. During the COVID-19 pandemic, there has been a dramatic rise in sales of supplements and vitamin C, during which time we observed an apparent increase in the proportion of ingestion-associated oxalate nephropathy.
Methods: We retrospectively reviewed secondary oxalate nephropathy and compared pre-pandemic (2018-2019) and pandemic (2020-early 2022) time periods.
Results: We identified 35 patients with kidney biopsy proven (30 native, 5 allograft) oxalate nephropathy at a single academic institution. Supplement-associated oxalate nephropathy comprised a significantly higher proportion of cases during COVID-19 pandemic compared with the preceding 2 years (44% vs. 0%, P = 0.002), and was associated with use of vitamin C, dietary changes, and supplements. Oxalate nephropathy in the kidney allograft, in contrast, remained associated with enteric hyperoxaluria, antibiotic use, and dehydration. Many patients had diabetes mellitus (57%), hypertension (40%) and/or pre-existing chronic kidney disease (CKD, 49%). Of 9 patients in which the potentially causative ingestion was identified and removed, 8 experienced improvement in kidney function.
Conclusion: There was a shift toward supplements rather than enteric hyperoxaluria as a leading cause of secondary oxalate nephropathy during the COVID-19 pandemic. Kidney outcomes are better than those observed for enteric hyperoxaluria, if the offending agent is identified and removed.
Keywords: COVID-19; SARS-CoV-2; gastric bypass; kidney biopsy; oxalate; vitamin C.
© 2022 International Society of Nephrology. Published by Elsevier Inc.
Figures

References
LinkOut - more resources
Full Text Sources
Miscellaneous
