

Association of State Child Abuse Policies and Mandated Reporting Policies With Prenatal and Postpartum Care Among Women Who Engaged in Substance Use During Pregnancy
- PMID: 36121649
- PMCID: PMC9486638
- DOI: 10.1001/jamapediatrics.2022.3396
Association of State Child Abuse Policies and Mandated Reporting Policies With Prenatal and Postpartum Care Among Women Who Engaged in Substance Use During Pregnancy
Abstract
Importance: Some states have implemented policies that consider substance use during pregnancy as child abuse and require mandated reporting of substance use during pregnancy. Implications of these policies for health care receipt among pregnant people who engage in substance use are unknown.
Objective: To examine the association of state child abuse policies and mandated reporting policies with prenatal and postpartum care among women who engaged in substance use during pregnancy.
Design, setting, and participants: In this cross-sectional study, data from the 2016-2019 Pregnancy Risk Assessment Monitoring System survey were analyzed. The study population included 4155 women from 23 states who reported substance use during pregnancy. Data were analyzed between August and November 2021.
Exposures: Delivery in a state with a child abuse policy only (n = 6), a mandated reporting policy only (n = 4), both policies (n = 7), or neither policy (n = 5). One state switched from a mandated reporting policy only to having both policies.
Main outcomes and measures: Month of gestation at prenatal care initiation (ie, months 1-10, with a higher number of months indicating later initiation), receipt of adequate prenatal care, and receipt of a postpartum health care visit 4 to 6 weeks after delivery. Sample characteristics were calculated using unweighted frequencies and weighted percentages and means. Associations of state policies with the outcomes were examined using generalized linear regression with generalized estimating equations, adjusting for potential confounders and accounting for the complex sampling design of the Pregnancy Risk Assessment Monitoring System survey.
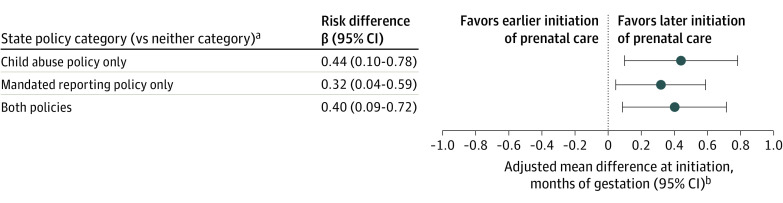
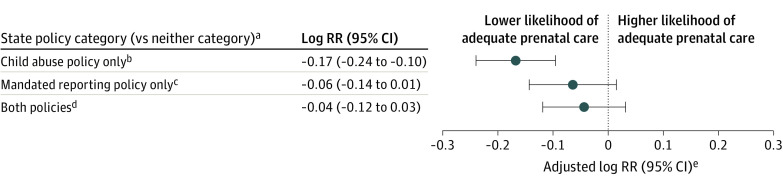
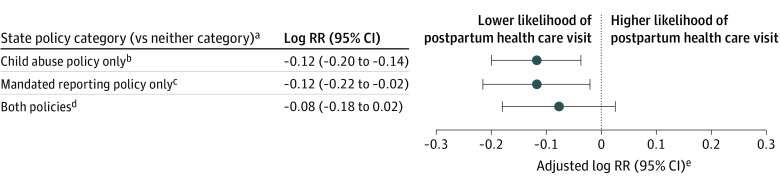
Results: The study sample included 4155 women who reported substance use during pregnancy; 33.9% of these women delivered in states with a child abuse policy only, 16.4% in states with a mandated reporting policy only, 32.9% in states with both policies, and 16.8% in states with neither policy. Overall, 14.7% of women were Black, 69.0% were White, and 64.6% were aged 18 to 29 years at delivery. Women who delivered in states with a child abuse policy only, mandated reporting policy only, or both policies initiated prenatal care at a later month of gestation (β = 0.44 [95% CI, 0.10-0.78], 0.32 [95% CI, 0.04-0.59], and 0.40 [95% CI, 0.09-0.72], respectively) and had a lower likelihood of adequate prenatal care (risk ratio, 0.85 [95% CI, 0.79-0.91], 0.94 [95% CI, 0.87-1.01], and 0.95 [95% CI, 0.89-1.03], respectively) and a postpartum health care visit (risk ratio, 0.89 [95% CI, 0.82-0.96], 0.89 [95% CI, 0.80-0.98], and 0.92 [95% CI, 0.83-1.02], respectively) compared with women who delivered in states with neither policy.
Conclusions and relevance: The results indicate that state child abuse policies and mandated reporting policies are associated with reduced receipt of prenatal and postpartum care among women who engage in substance use during pregnancy.
Conflict of interest statement
Figures
Comment in
-
Mandated Reporting of Perinatal Substance Use: The Root of Inequity.JAMA Pediatr. 2022 Nov 1;176(11):1073-1075. doi: 10.1001/jamapediatrics.2022.3404. JAMA Pediatr. 2022. PMID: 36121662 No abstract available.
References
-
- 2020 National Survey on Drug Use and Health (NSDUH) Releases. Substance Abuse and Mental Health Services Administration . 2021. Accessed May 6, 2022. https://www.samhsa.gov/data/release/2020-national-survey-drug-use-and-he...
