

Association of Early Oseltamivir With Improved Outcomes in Hospitalized Children With Influenza, 2007-2020
- PMID: 36121673
- PMCID: PMC9486642
- DOI: 10.1001/jamapediatrics.2022.3261
Association of Early Oseltamivir With Improved Outcomes in Hospitalized Children With Influenza, 2007-2020
Abstract
Importance: Oseltamivir is recommended for all children hospitalized with influenza, despite limited evidence supporting its use in the inpatient setting.
Objective: To determine whether early oseltamivir use is associated with improved outcomes in children hospitalized with influenza.
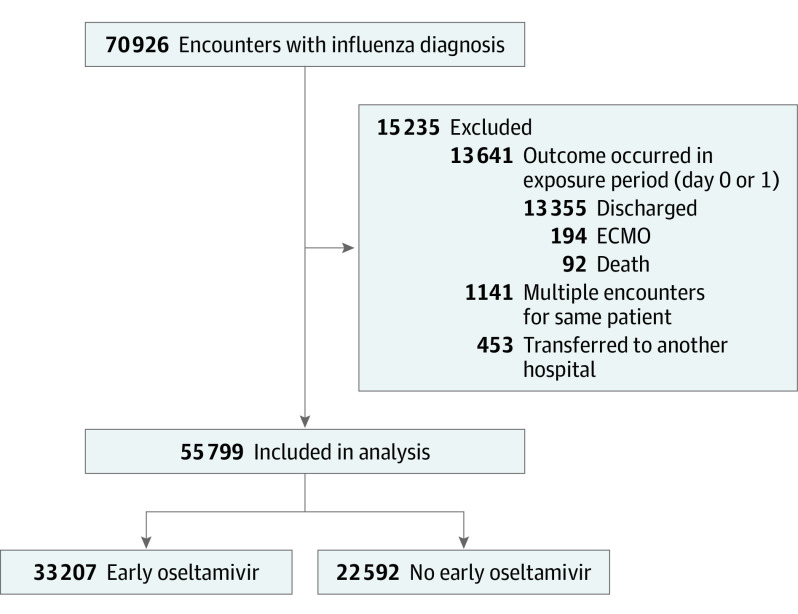
Design, setting, and participants: This multicenter retrospective study included 55 799 children younger than 18 years who were hospitalized with influenza from October 1, 2007, to March 31, 2020, in 36 tertiary care pediatric hospitals who participate in the Pediatric Health Information System database. Data were analyzed from January 2021 to March 2022.
Exposures: Early oseltamivir treatment, defined as use of oseltamivir on hospital day 0 or 1.
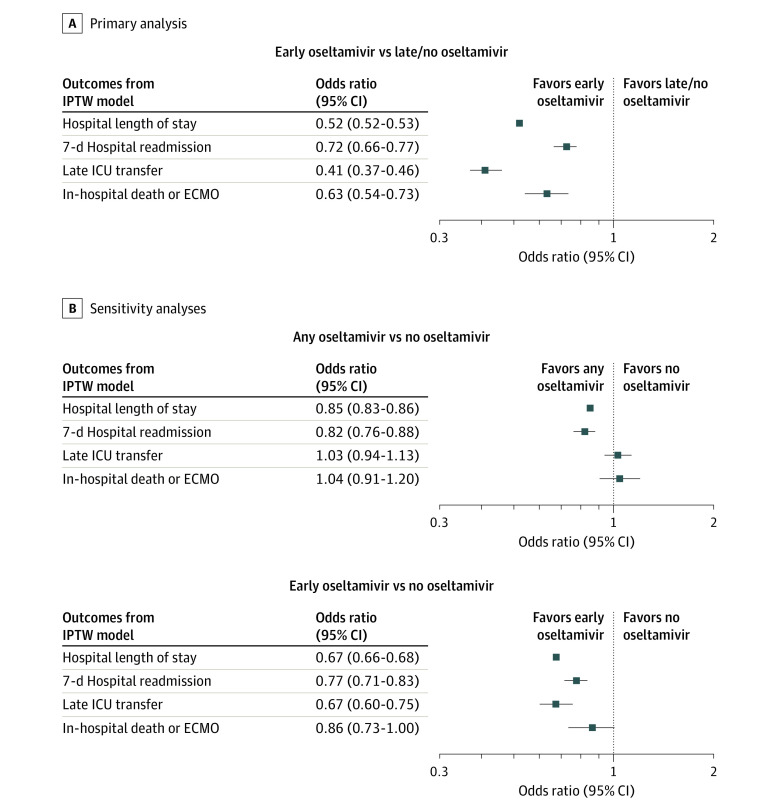
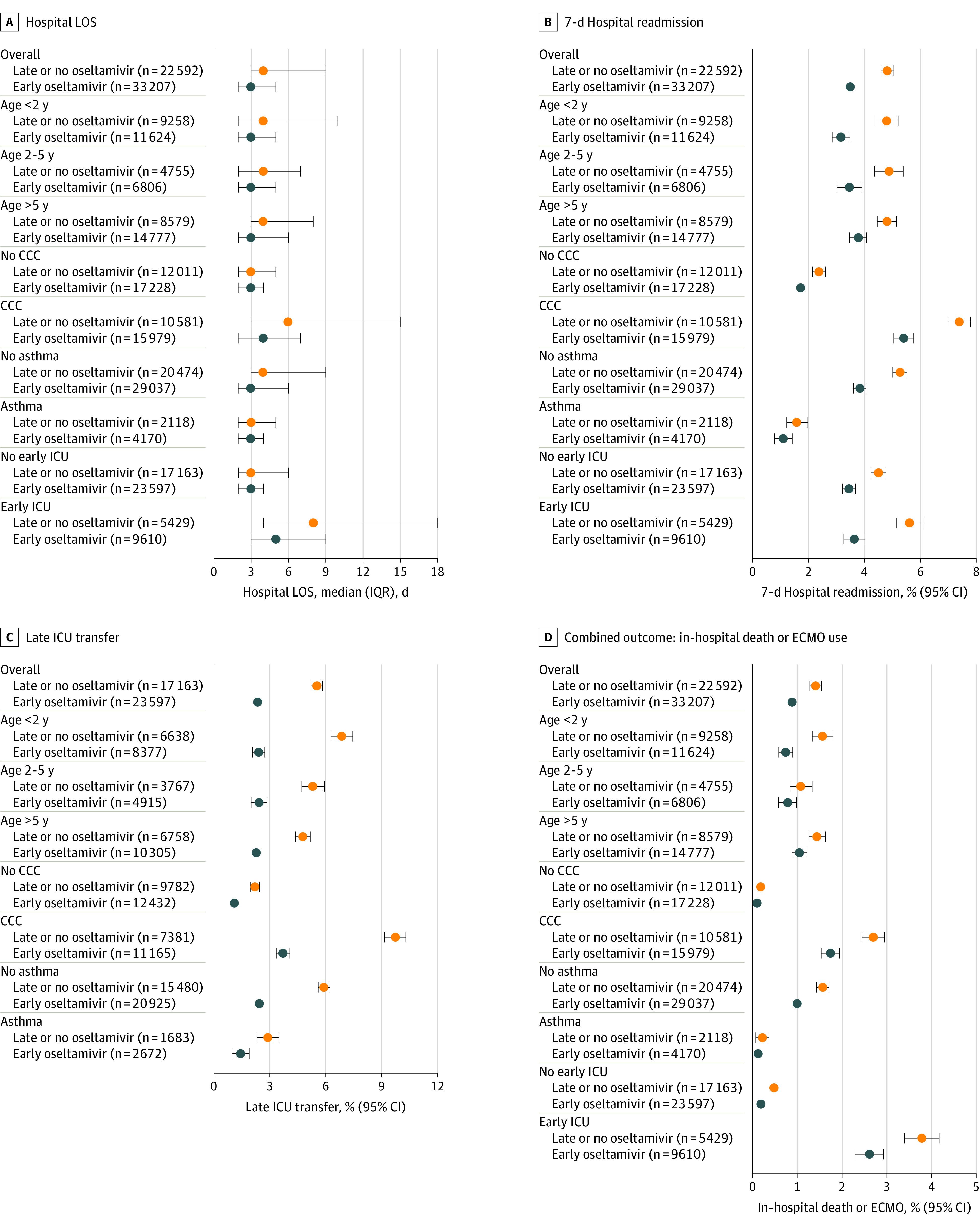
Main outcomes and measures: The primary outcome was hospital length of stay (LOS) in calendar days. Secondary outcomes included 7-day hospital readmission, late (hospital day 2 or later) intensive care unit (ICU) transfer, and a composite outcome of in-hospital death or use of extracorporeal membrane oxygenation (ECMO). Inverse probability treatment weighting (IPTW) based on propensity scoring was used to address confounding by indication. Mixed-effects models were used to compare outcomes between children who did and did not receive early oseltamivir treatment. Outcomes were also compared within high-risk subgroups based on age, presence of a complex chronic condition, early critical illness, and history of asthma.
Results: The analysis included 55 799 encounters from 36 hospitals. The median (IQR) age of the cohort was 3.61 years (1.03-8.27); 56% were male, and 44% were female. A total of 33 207 patients (59.5%) received early oseltamivir. In propensity score-weighted models, we found that children treated with early oseltamivir had shorter LOS (median 3 vs 4 days; IPTW model ratio, 0.52; 95% CI, 0.52-0.53) and lower odds of all-cause 7-day hospital readmission (3.5% vs 4.8%; adjusted odds ratio [aOR], 0.72; 95% CI, 0.66-0.77), late ICU transfer (2.4% vs 5.5%; aOR, 0.41; 95% CI, 0.37-0.46), and the composite outcome of death or ECMO use (0.9% vs 1.4%; aOR, 0.63; 95% CI, 0.54-0.73).
Conclusions and relevance: Early use of oseltamivir in hospitalized children was associated with shorter hospital stay and lower odds of 7-day readmission, ICU transfer, ECMO use, and death. These findings support the current recommendations for oseltamivir use in children hospitalized with influenza.
Conflict of interest statement
Figures
References
-
- Harper SA, Bradley JS, Englund JA, et al. ; Expert Panel of the Infectious Diseases Society of America . Seasonal influenza in adults and children--diagnosis, treatment, chemoprophylaxis, and institutional outbreak management: clinical practice guidelines of the Infectious Diseases Society of America. Clin Infect Dis. 2009;48(8):1003-1032. doi:10.1086/598513 - DOI - PMC - PubMed
Publication types
MeSH terms
Substances
LinkOut - more resources
Full Text Sources
Medical
