

Association of COVID-19 With Major Arterial and Venous Thrombotic Diseases: A Population-Wide Cohort Study of 48 Million Adults in England and Wales
- PMID: 36121907
- PMCID: PMC9484653
- DOI: 10.1161/CIRCULATIONAHA.122.060785
Association of COVID-19 With Major Arterial and Venous Thrombotic Diseases: A Population-Wide Cohort Study of 48 Million Adults in England and Wales
Abstract
Background: Infection with severe acute respiratory syndrome coronavirus 2 (SARS-CoV-2) induces a prothrombotic state, but long-term effects of COVID-19 on incidence of vascular diseases are unclear.
Methods: We studied vascular diseases after COVID-19 diagnosis in population-wide anonymized linked English and Welsh electronic health records from January 1 to December 7, 2020. We estimated adjusted hazard ratios comparing the incidence of arterial thromboses and venous thromboembolic events (VTEs) after diagnosis of COVID-19 with the incidence in people without a COVID-19 diagnosis. We conducted subgroup analyses by COVID-19 severity, demographic characteristics, and previous history.
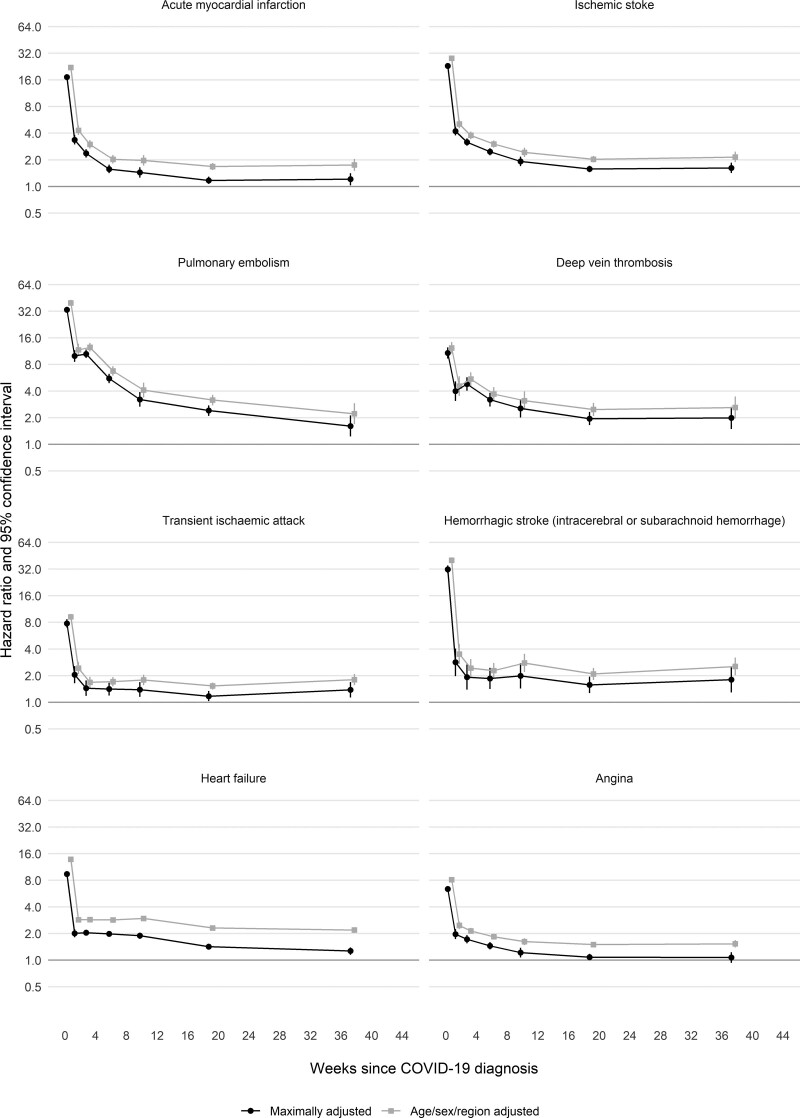
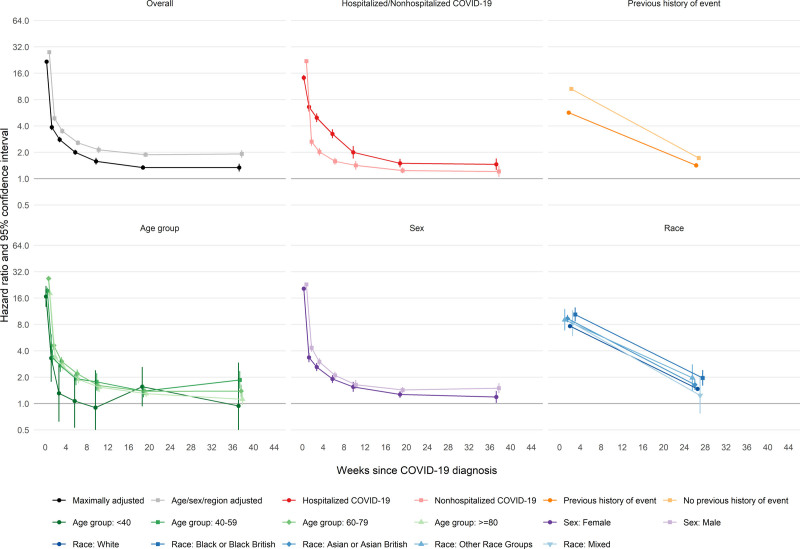
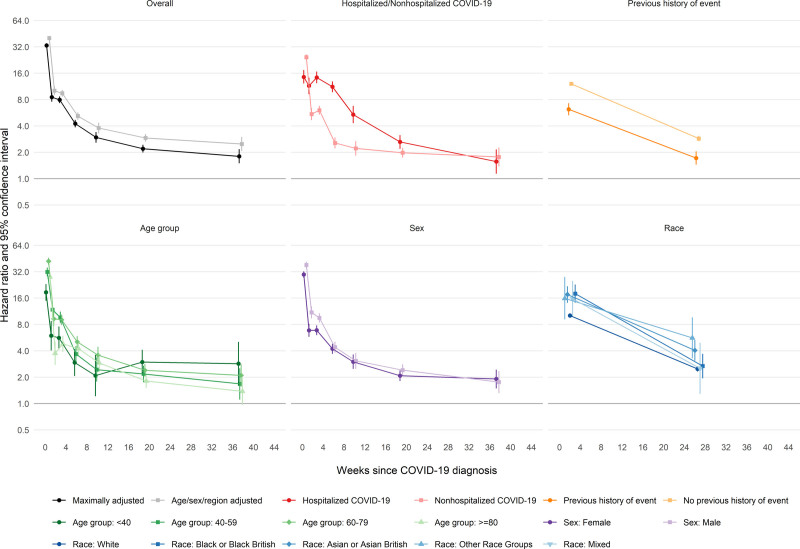
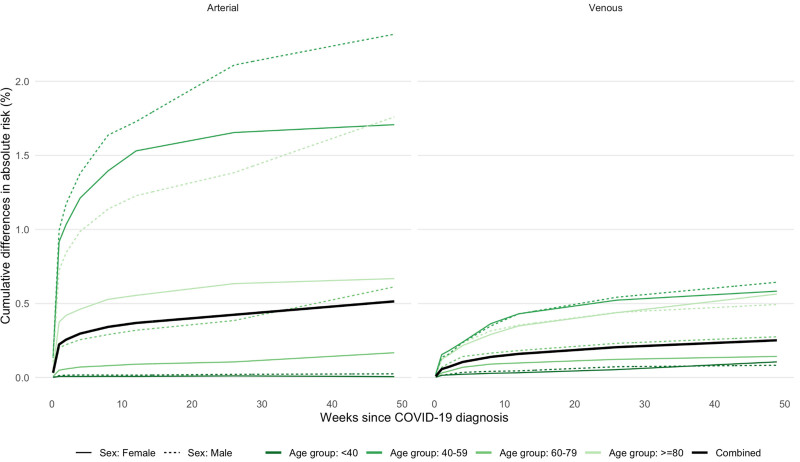
Results: Among 48 million adults, 125 985 were hospitalized and 1 319 789 were not hospitalized within 28 days of COVID-19 diagnosis. In England, there were 260 279 first arterial thromboses and 59 421 first VTEs during 41.6 million person-years of follow-up. Adjusted hazard ratios for first arterial thrombosis after COVID-19 diagnosis compared with no COVID-19 diagnosis declined from 21.7 (95% CI, 21.0-22.4) in week 1 after COVID-19 diagnosis to 1.34 (95% CI, 1.21-1.48) during weeks 27 to 49. Adjusted hazard ratios for first VTE after COVID-19 diagnosis declined from 33.2 (95% CI, 31.3-35.2) in week 1 to 1.80 (95% CI, 1.50-2.17) during weeks 27 to 49. Adjusted hazard ratios were higher, for longer after diagnosis, after hospitalized versus nonhospitalized COVID-19, among Black or Asian versus White people, and among people without versus with a previous event. The estimated whole-population increases in risk of arterial thromboses and VTEs 49 weeks after COVID-19 diagnosis were 0.5% and 0.25%, respectively, corresponding to 7200 and 3500 additional events, respectively, after 1.4 million COVID-19 diagnoses.
Conclusions: High relative incidence of vascular events soon after COVID-19 diagnosis declines more rapidly for arterial thromboses than VTEs. However, incidence remains elevated up to 49 weeks after COVID-19 diagnosis. These results support policies to prevent severe COVID-19 by means of COVID-19 vaccines, early review after discharge, risk factor control, and use of secondary preventive agents in high-risk patients.
Keywords: COVID-19; electronic health records; myocardial infarction; pulmonary embolism; stroke; thrombosis; venous thrombosis.
Figures
References
-
- Loo J, Spittle DA, Newnham M. COVID-19, immunothrombosis and venous thromboembolism: biological mechanisms. Thorax. 2021;76:412–420. doi: 10.1136/thoraxjnl-2020-216243 - PubMed
-
- Hippisley-Cox J, Patone M, Mei XW, Saatci D, Dixon S, Khunti K, Zaccardi F, Watkinson P, Shankar-Hari M, Doidge J, et al. Risk of thrombocytopenia and thromboembolism after covid-19 vaccination and SARS-CoV-2 positive testing: self-controlled case series study. BMJ. 2021;374:n1931. doi: 10.1136/bmj.n1931 - PMC - PubMed
Publication types
MeSH terms
Substances
Grants and funding
LinkOut - more resources
Full Text Sources
Other Literature Sources
Medical
Miscellaneous
