

Review of potential medical treatments for middle ear cholesteatoma
- PMID: 36123729
- PMCID: PMC9487140
- DOI: 10.1186/s12964-022-00953-w
Review of potential medical treatments for middle ear cholesteatoma
Abstract
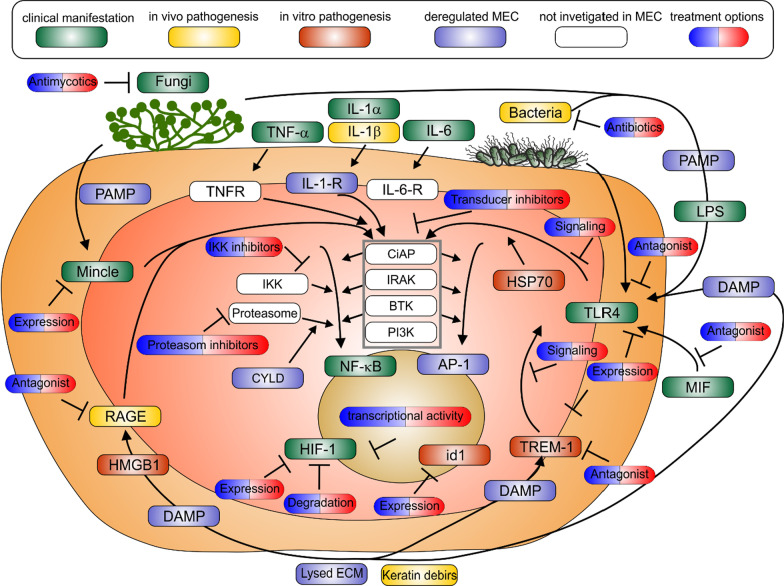
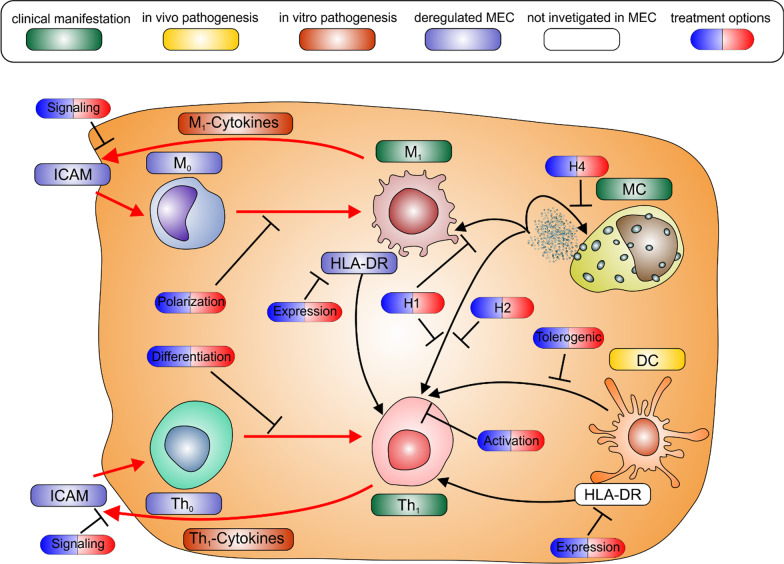
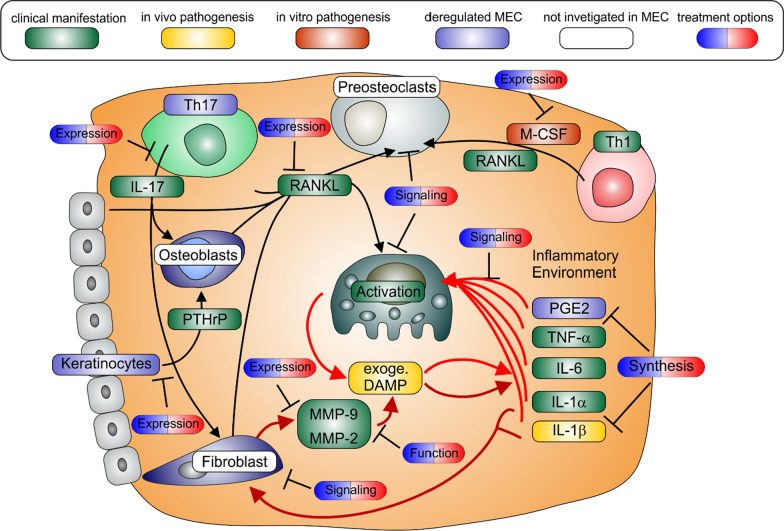
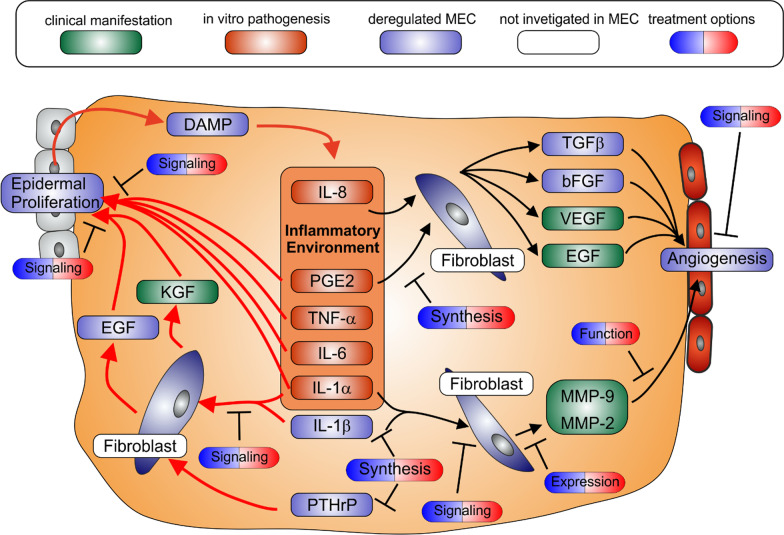
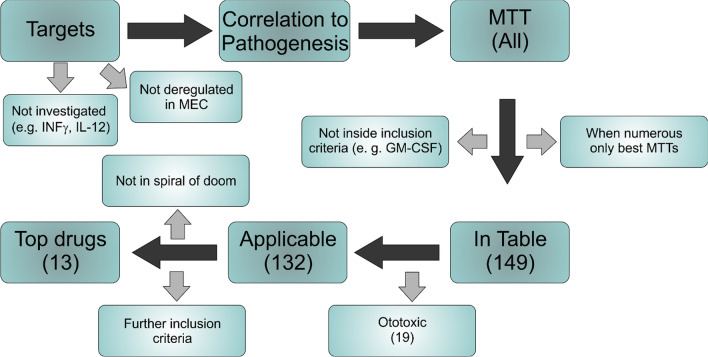
Middle ear cholesteatoma (MEC), is a destructive, and locally invasive lesion in the middle ear driven by inflammation with an annual incidence of 10 per 100,000. Surgical extraction/excision remains the only treatment strategy available and recurrence is high (up to 40%), therefore developing the first pharmaceutical treatments for MEC is desperately required. This review was targeted at connecting the dysregulated inflammatory network of MEC to pathogenesis and identification of pharmaceutical targets. We summarized the numerous basic research endeavors undertaken over the last 30+ years to identify the key targets in the dysregulated inflammatory pathways and judged the level of evidence for a given target if it was generated by in vitro, in vivo or clinical experiments. MEC pathogenesis was found to be connected to cytokines characteristic for Th1, Th17 and M1 cells. In addition, we found that the inflammation created damage associated molecular patterns (DAMPs), which further promoted inflammation. Similar positive feedback loops have already been described for other Th1/Th17 driven inflammatory diseases (arthritis, Crohn's disease or multiple sclerosis). A wide-ranging search for molecular targeted therapies (MTT) led to the discovery of over a hundred clinically approved drugs already applied in precision medicine. Based on exclusion criteria designed to enable fast translation as well as efficacy, we condensed the numerous MTTs down to 13 top drugs. The review should serve as groundwork for the primary goal, which is to provide potential pharmaceutical therapies to MEC patients for the first time in history. Video Abstract.
Keywords: Adaptive immune response; Cholesteatoma; Chronic inflammation; Innate immune system; Positive feedback loops; Precision medicine.
Plain language summary
Middle ear cholesteatoma (MEC) is a destructive and locally invasive ulcerated lesion in the middle ear driven by inflammation which occurs in 10 out of 100,000 people annually. Surgical extraction/excision is the only treatment strategy available and recurrence is high (up to 40% after ten years), therefore developing the first pharmaceutical treatments for MEC is desperately required. This review is focused on the connections between inflammation and MEC pathogenesis. These connections can be used as attack points for pharmaceuticals. For this we summarized the results of research undertaken over the last 30 + years. MEC pathogenesis can be described by specific inflammatory dysregulation already known from arthritis, Crohn’s disease or multiple sclerosis. A hallmark of this dysregulation are positive feedback loops of the inflammation further amplifying itself in a vicious circle-like manner. We have identified over one hundred drugs which are already used in clinic to treat other inflammatory diseases, and could potentially be repurposed to treat MEC. To improve and expedite clinical success rates, we applied certain criteria based on our literature searches and condensed these drugs down to the 13 top drugs. We hope the review will serve as groundwork for the primary goal, which is to provide potential pharmaceutical therapies to MEC patients for the first time in history.
© 2022. The Author(s).
Conflict of interest statement
The authors declare that they have no competing interests.
Figures
References
Publication types
MeSH terms
Substances
LinkOut - more resources
Full Text Sources
