

Human Cardiac Pericytes Are Susceptible to SARS-CoV-2 Infection
- PMID: 36124009
- PMCID: PMC9473702
- DOI: 10.1016/j.jacbts.2022.09.001
Human Cardiac Pericytes Are Susceptible to SARS-CoV-2 Infection
Abstract
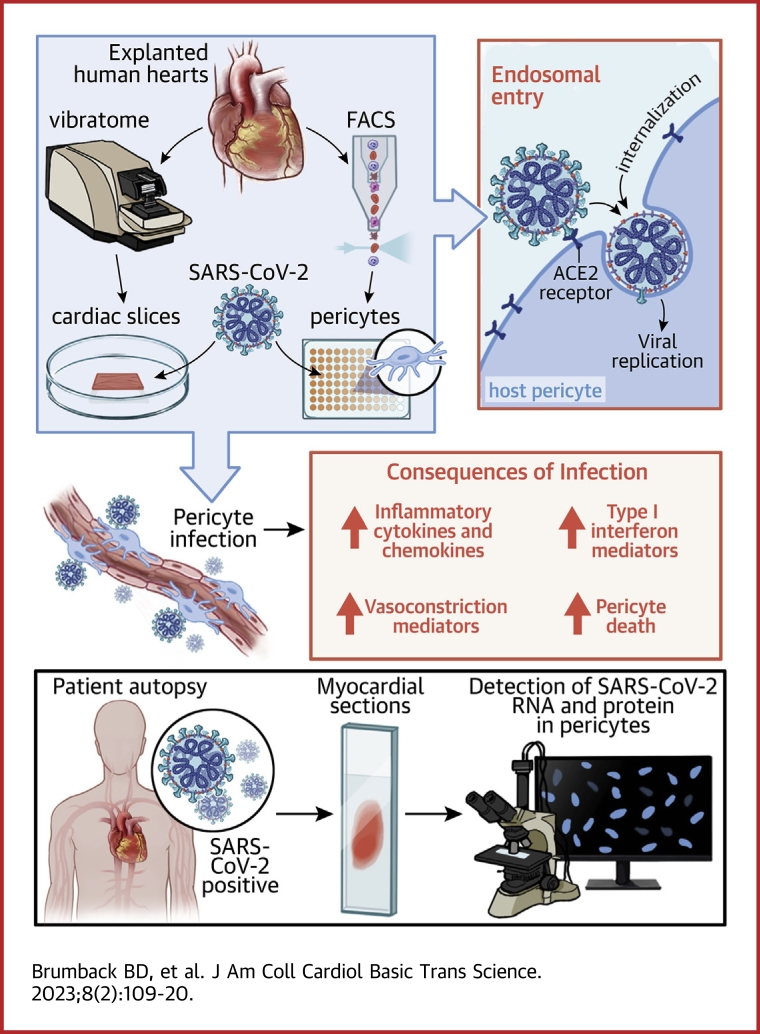
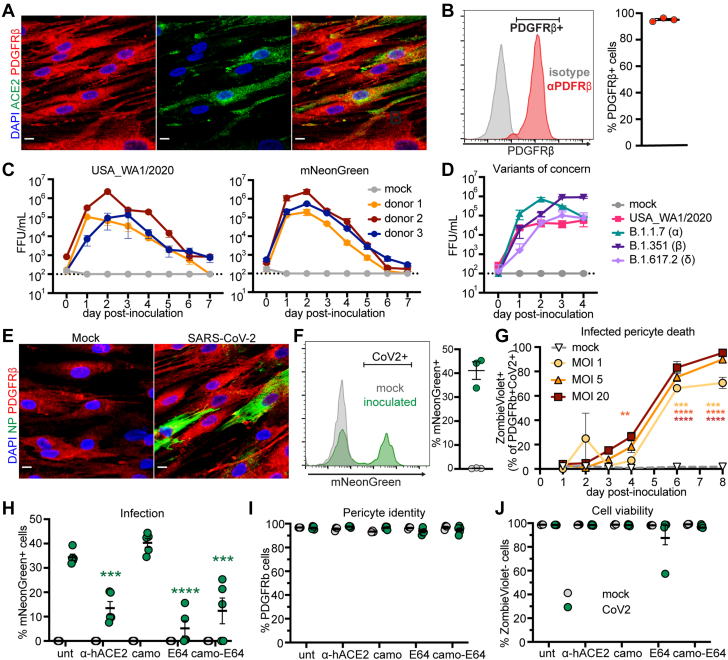
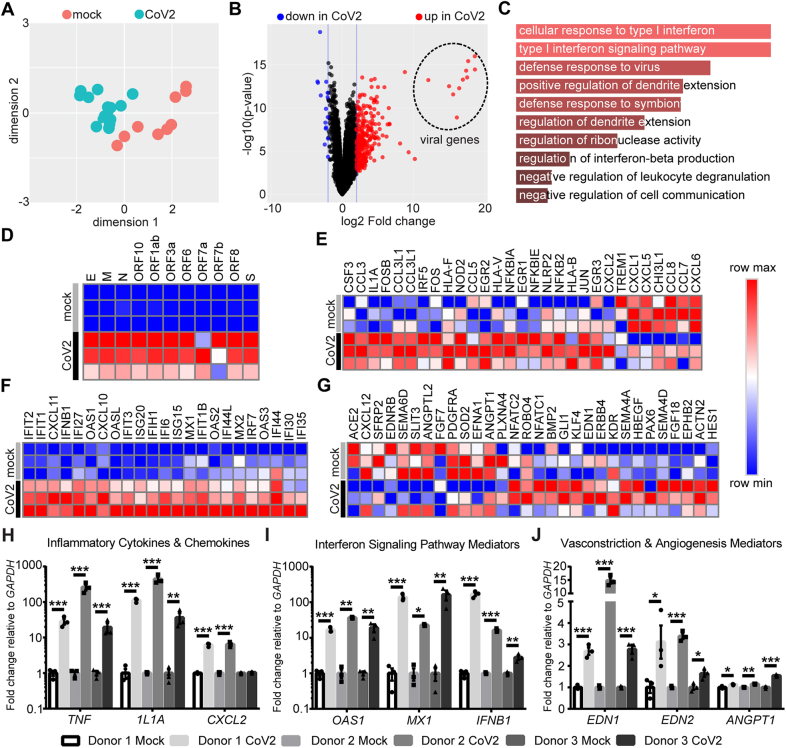
COVID-19 is associated with serious cardiovascular complications, with incompletely understood mechanism(s). Pericytes have key functions in supporting endothelial cells and maintaining vascular integrity. We demonstrate that human cardiac pericytes are permissive to SARS-CoV-2 infection in organotypic slice and primary cell cultures. Viral entry into pericytes is mediated by endosomal proteases, and infection leads to up-regulation of inflammatory markers, vasoactive mediators, and nuclear factor kappa-B-dependent cell death. Furthermore, we present evidence of cardiac pericyte infection in COVID-19 myocarditis patients. These data demonstrate that human cardiac pericytes are susceptible to SARS-CoV-2 infection and suggest a role for pericyte infection in COVID-19.
Keywords: ACE2, angiotensin-converting enzyme 2; COVID-19; IFN, interferon; MOI, multiplicity of infection; PDGFRβ, platelet-derived growth factor receptor beta; SARS-CoV-2; cardiovascular disease; pericytes.
© 2023 The Authors.
Conflict of interest statement
This research was supported by National Institutes of Health/National Center for Advancing Translational Sciences grant UH3 HL141800-04S1 COVID-19 supplement for an emergency response to COVID-19 (to Dr Rentschler), National Institutes of Health National Heart, Lung, and Blood Institute/National Center for Advancing Translational Sciences UH3 HL 141800 (to Dr Rentschler), and the National Science Foundation GRFP grant DGE-1745038 (to Dr Brumback). The Genome Technology Access Center at the McDonnell Genome Institute at Washington University School of Medicine is partially supported by NCI Cancer Center Support Grant #P30 CA91842 to the Siteman Cancer Center and by ICTS/CTSA Grant# UL1TR002345 from the National Center for Research Resources, a component of the National Institutes of Health, and National Institutes of Health Roadmap for Medical Research. Dr Diamond is supported by the National Institutes of Health (R01 AI157155); is a consultant for Inbios, Vir Biotechnology, Moderna, Immunome, and Senda Biosciences; and has received unrelated sponsored research agreement funding from Moderna, Vir Biotechnology, and Emergent BioSolutions. Dr Lavine is supported by the National Institutes of Health (R01 HL138466, R01 HL139714, R01 HL151078), Leducq Foundation Network (#20CVD02), Burroughs Wellcome Fund (1014782), Children’s Discovery Institute of Washington University and St. Louis Children’s Hospital (CH-II-2015-462, CH-II-2017-628, PM-LI-2019-829), and Foundation of Barnes-Jewish Hospital (8038-88); is a consultant for Implicit Biosciences and Flame Biosciences; is a member of the Medtronic: DT-PAS/APOGEE trial advisory board; and has received funding and unrelated sponsored research agreements from Amgen and Novartis. Dr Rentschler is supported by the National Institutes of Health (R01 HL130212, UH3 HL141800), Burroughs Wellcome Fund (1009884), Foundation of Barnes-Jewish Hospital, and Additional Ventures Cures Collaborative. All other authors have reported that they have no relationships relevant to the contents of this paper to disclose.
Figures


Comment in
-
Cardiac Pericytes: Underappreciated Targets of SARS-CoV-2.JACC Basic Transl Sci. 2023 Feb;8(2):121-123. doi: 10.1016/j.jacbts.2023.01.010. Epub 2023 Feb 27. JACC Basic Transl Sci. 2023. PMID: 36875780 Free PMC article.
References
-
- Pellegrini D., Kawakami R., Guagliumi G., et al. Microthrombi as a major cause of cardiac injury in COVID-19: a pathologic study. Circulation. 2021;143:1031–1042. - PubMed
Grants and funding
LinkOut - more resources
Full Text Sources
Molecular Biology Databases
Miscellaneous
