

There is urgent need to treat atherosclerotic cardiovascular disease risk earlier, more intensively, and with greater precision: A review of current practice and recommendations for improved effectiveness
- PMID: 36124049
- PMCID: PMC9482082
- DOI: 10.1016/j.ajpc.2022.100371
There is urgent need to treat atherosclerotic cardiovascular disease risk earlier, more intensively, and with greater precision: A review of current practice and recommendations for improved effectiveness
Abstract
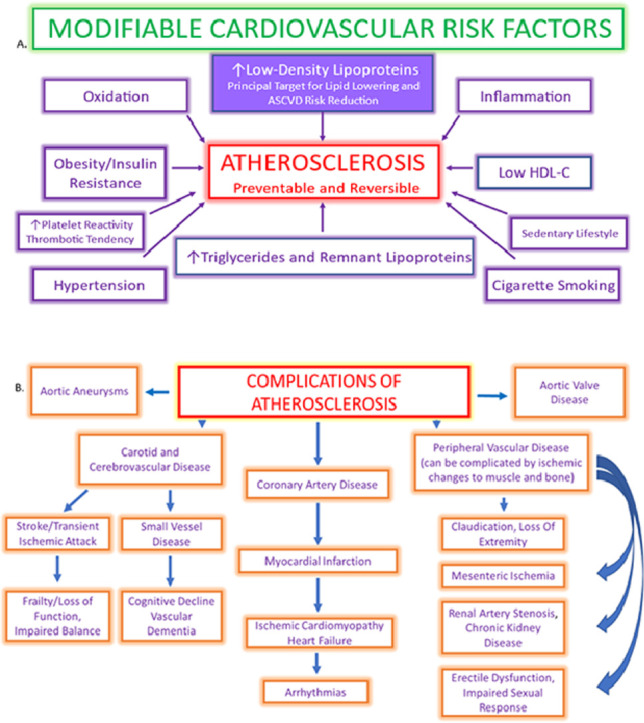
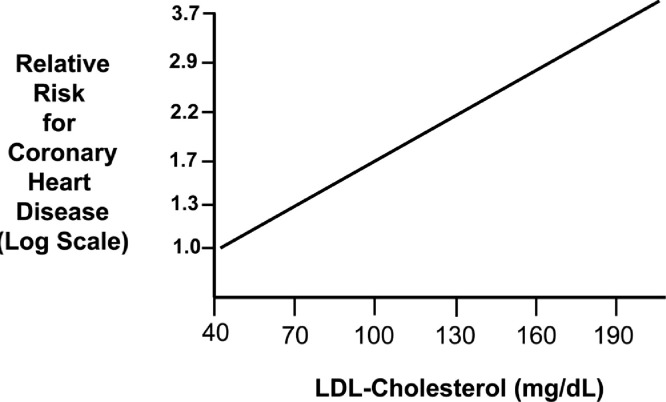
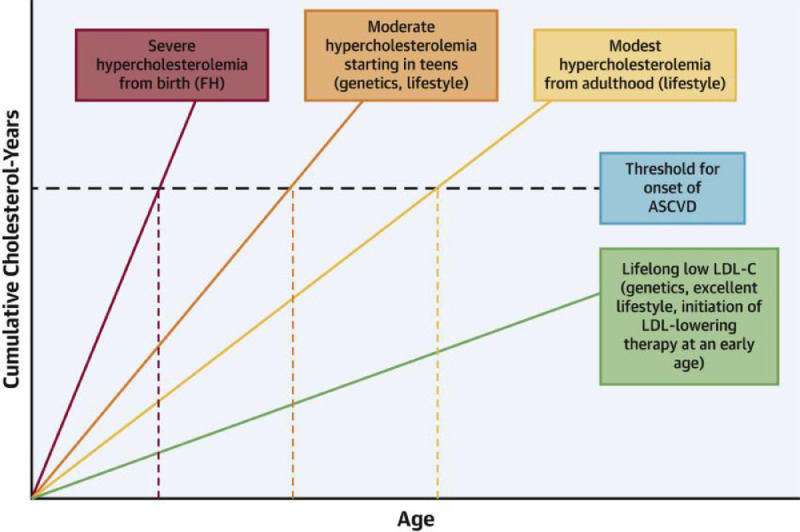
Atherosclerotic cardiovascular disease (ASCVD) is epidemic throughout the world and is etiologic for such acute cardiovascular events as myocardial infarction, ischemic stroke, unstable angina, and death. ASCVD also impacts risk for dementia, chronic kidney disease peripheral arterial disease and mobility, impaired sexual response, and a host of other visceral impairments that adversely impact the quality and rate of progression of aging. The relationship between low-density lipoprotein cholesterol (LDL-C) and risk for ASCVD is one of the most highly established and investigated issues in the entirety of modern medicine. Elevated LDL-C is a necessary condition for atherogenesis induction. Basic scientific investigation, prospective longitudinal cohorts, and randomized clinical trials have all validated this association. Yet despite the enormous number of clinical trials which support the need for reducing the burden of atherogenic lipoprotein in blood, the percentage of high and very high-risk patients who achieve risk stratified LDL-C target reductions is low and has remained low for the last thirty years. Atherosclerosis is a preventable disease. As clinicians, the time has come for us to take primordial and primary prevention more serously. Despite a plethora of therapeutic approaches, the large majority of patients at risk for ASCVD are poorly or inadequately treated, leaving them vulnerable to disease progression, acute cardiovascular events, and poor aging due to loss of function in multiple visceral organs. Herein we discuss the need to greatly intensify efforts to reduce risk, decrease disease burden, and provide more comprehensive and earlier risk assessment to optimally prevent ASCVD and its complications. Evidence is presented to support that treatment should aim for far lower goals in cholesterol management, should take into account many more factors than commonly employed today and should begin significantly earlier in life.
Keywords: ASCVD, Atherosclerotic cardiovascular disease; Atherosclerosis; CAC, Coronary artery calcium; CAD, coronary artery disease; CCTA, Coronary computed tomographic angiography; CHD, Coronary Heart Disease; Cholesterol; Coronary artery disease; Dementia; FCT, Fibrous Cap Thickness; FH, Familial hypercholesterolemia; HDL-C, High-density lipoprotein cholesterol; HMG CoA, 3-hydroxymethyl-3-methylglutaryl coenzyme A; IDL, Intermediate-density lipoprotein; LCBI, Lipid core burden index; LDL-C, low-density lipoprotein cholesterol; LLT, Lipid-lowering therapy; Lipoproteins; MCI, Mild cognitive impairment; MI, myocardial infarction; Myocardial infarction; NFT, Neurofibrillary tangle; NMR, Nuclear Magnetic Resonance; NPV, Negative predictive value; PAD, Peripheral Arterial Disease; PAV, Percent Atheroma Volume; PCSK9, Proprotein convertase subtilisin:kexin type 9; Prevention; RCT, Randomized controlled trial; Stroke; VLDL, Very low-density lipoprotein; apoB, apolipoprotein B.
© 2022 The Authors. Published by Elsevier B.V.
Conflict of interest statement
Michael Makover: None. Michael Shapiro: Dr Shapiro has participated in the Scientific Advisory Boards for Amgen, Esperion, Novartis, and Novo Nordisk. Peter P. Toth: Dr. Toth is a member of the speakers bureau for Amarin, Amgen, Esperion, and Novo-Nordisk; he is a consultant to Amarin, Kowa, Merck, Novartis, and Resverlogix.
Figures
References
-
- Song P., Fang Z., Wang H., et al. Global and regional prevalence, burden, and risk factors for carotid atherosclerosis: a systematic review, meta-analysis, and modelling study. Lancet Glob Health. 2020;8:e721–e729. - PubMed
-
- Jr. MLk. Beyond Vietnam: A Time to Break the Silence. Addressing a crowd of 3,000 at Riverside Church in New York City. 1967.
-
- Ford E.S., Capewell S. Proportion of the decline in cardiovascular mortality disease due to prevention versus treatment: public health versus clinical care. Annu Rev Public Health. 2011;32:5–22. - PubMed
Publication types
LinkOut - more resources
Full Text Sources
Medical
Research Materials
Miscellaneous
