

Impact on right ventricular performance in patients undergoing permanent pacemaker implantation: Left bundle branch pacing versus right ventricular septum pacing
- PMID: 36124394
- PMCID: PMC10091979
- DOI: 10.1111/jce.15675
Impact on right ventricular performance in patients undergoing permanent pacemaker implantation: Left bundle branch pacing versus right ventricular septum pacing
Abstract
Background: The novel method of left bundle branch pacing (LBBP) has been reported to achieve better electrical and mechanical synchrony in the left ventricle than conventional right ventricular pacing (RVP). However, its effects on right ventricle (RV) performance are still unknown.
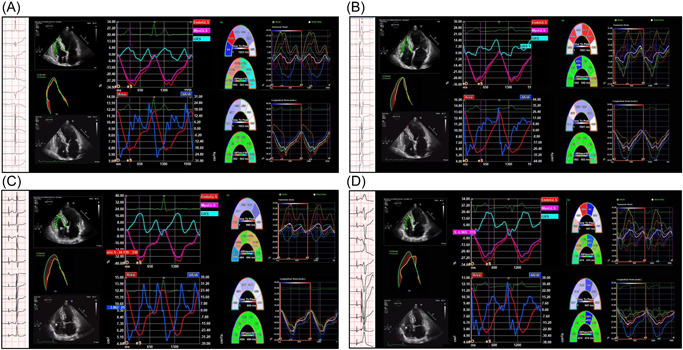
Methods: Consecutive patients undergoing dual-chamber pacemaker (PM) implantation for sick sinus syndrome (SSS) with normal cardiac function and a narrow QRS complex were recruited for the study. The pacing characteristics and echocardiogram parameters were measured to evaluate RV function, interventricular and RV synchrony, and were compared between ventricular pacing-on and native-conduction modes.
Results: A total of 84 patients diagnosed with SSS and an indication for pacing therapy were enrolled. Forty-two patients (50%; mean age 65.50 ± 9.30 years; 35% male) underwent successful LBBP and 42 patients (50%; mean age 69.26 ± 10.08 years; 33% male) RVSP, respectively. Baseline characteristics were similar between the two groups. We found no significant differences in RV function [RV-FAC (Fractional Area Change)%, 47.13 ± 5.69 versus 48.60 ± 5.83, p = .069; Endo-GLS (Global Longitudinal Strain)%, -28.88 ± 4.94 versus -29.82 ± 5.35, p = .114; Myo-GLS%, -25.72 ± 4.75 versus -25.72 ± 5.21, p = .559; Free Wall St%, 27.40 ± 8.03 versus -28.71 ± 7.34, p = .304] between the native-conduction and LBBP capture modes, while the RVSP capture mode was associated with a significant reduction in the above parameters compared with the native-conduction mode (p < .0001). The interventricular synchrony in the LBBP group was also superior to the RVSP group significantly.
Conclusion: LBBP is a pacing technique that seems to associate with a positive and protective impact on RV performance.
Keywords: cardiac mechanical synchrony; echocardiography; left bundle branch pacing; physiological pacing; right ventricular function; right ventricular septum pacing; sick sinus syndrome.
© 2022 The Authors. Journal of Cardiovascular Electrophysiology published by Wiley Periodicals LLC.
Figures



Similar articles
-
Evaluation of cardiac synchrony in left bundle branch pacing: Insights from echocardiographic research.J Cardiovasc Electrophysiol. 2020 Feb;31(2):560-569. doi: 10.1111/jce.14342. Epub 2020 Jan 20. J Cardiovasc Electrophysiol. 2020. PMID: 31919928 Free PMC article.
-
Evaluation of electrophysiological characteristics and ventricular synchrony: An intrapatient-controlled study during His-Purkinje conduction system pacing versus right ventricular pacing.Clin Cardiol. 2022 Jul;45(7):723-732. doi: 10.1002/clc.23837. Epub 2022 May 3. Clin Cardiol. 2022. PMID: 35502628 Free PMC article.
-
Feasibility and cardiac synchrony of permanent left bundle branch pacing through the interventricular septum.Europace. 2019 Nov 1;21(11):1694-1702. doi: 10.1093/europace/euz188. Europace. 2019. PMID: 31322651
-
Safety and efficacy of left bundle branch pacing in comparison with conventional right ventricular pacing: A systematic review and meta-analysis.Medicine (Baltimore). 2021 Jul 9;100(27):e26560. doi: 10.1097/MD.0000000000026560. Medicine (Baltimore). 2021. PMID: 34232199 Free PMC article.
-
How to implant left bundle branch pacing lead in routine clinical practice.J Cardiovasc Electrophysiol. 2019 Nov;30(11):2569-2577. doi: 10.1111/jce.14190. Epub 2019 Sep 26. J Cardiovasc Electrophysiol. 2019. PMID: 31535747 Review.
Cited by
-
Comparison between left bundle branch area pacing and right ventricular pacing: ventricular electromechanical synchrony and risk of atrial high-rate episodes.Front Cardiovasc Med. 2024 Apr 25;11:1267076. doi: 10.3389/fcvm.2024.1267076. eCollection 2024. Front Cardiovasc Med. 2024. PMID: 38725829 Free PMC article.
-
A systematic review and meta-analysis of the impact of left bundle branch area pacing on right ventricular function.Front Cardiovasc Med. 2025 Jan 30;12:1545757. doi: 10.3389/fcvm.2025.1545757. eCollection 2025. Front Cardiovasc Med. 2025. PMID: 39981350 Free PMC article.
-
Enhanced ventricular synchrony and myocardial function with bipolar left bundle area pacing: a comparative study of anodal ring capture versus unipolar pacing.Eur Heart J Open. 2025 Jun 18;5(3):oeaf077. doi: 10.1093/ehjopen/oeaf077. eCollection 2025 May. Eur Heart J Open. 2025. PMID: 40584584 Free PMC article.
-
Evaluation of Right Heart Structure and Function in Pacemaker-dependent Patients by Two-Dimensional Speckle Tracking Echocardiography: A 1-Year Prospective Cohort Study.Rev Cardiovasc Med. 2024 Nov 20;25(11):408. doi: 10.31083/j.rcm2511408. eCollection 2024 Nov. Rev Cardiovasc Med. 2024. PMID: 39618867 Free PMC article.
References
Publication types
MeSH terms
LinkOut - more resources
Full Text Sources
Medical
Miscellaneous
