

Benefit of Risk-stratified Prophylactic Treatment on Clinical Outcome in Postoperative Crohn's Disease
- PMID: 36124739
- PMCID: PMC10069621
- DOI: 10.1093/ecco-jcc/jjac139
Benefit of Risk-stratified Prophylactic Treatment on Clinical Outcome in Postoperative Crohn's Disease
Abstract
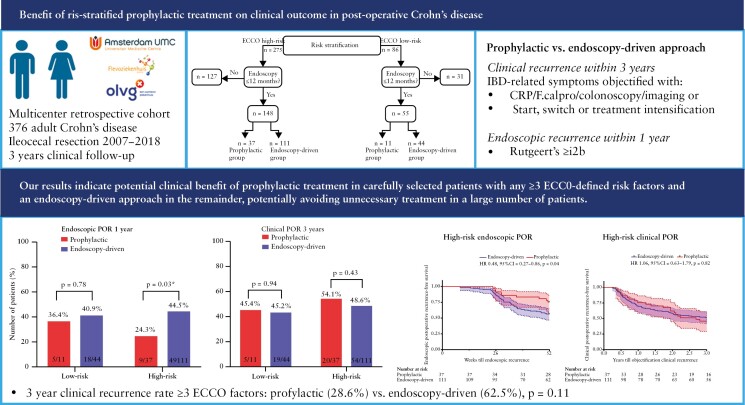
Background and aims: Whereas immediate postoperative treatment has shown effectiveness in reducing endoscopic postoperative recurrence [POR], evidence regarding the clinical benefit is limited. We compared rates of clinical POR in Crohn's disease [CD] patients receiving immediate prophylactic treatment with rates in patients receiving endoscopy-driven treatment.
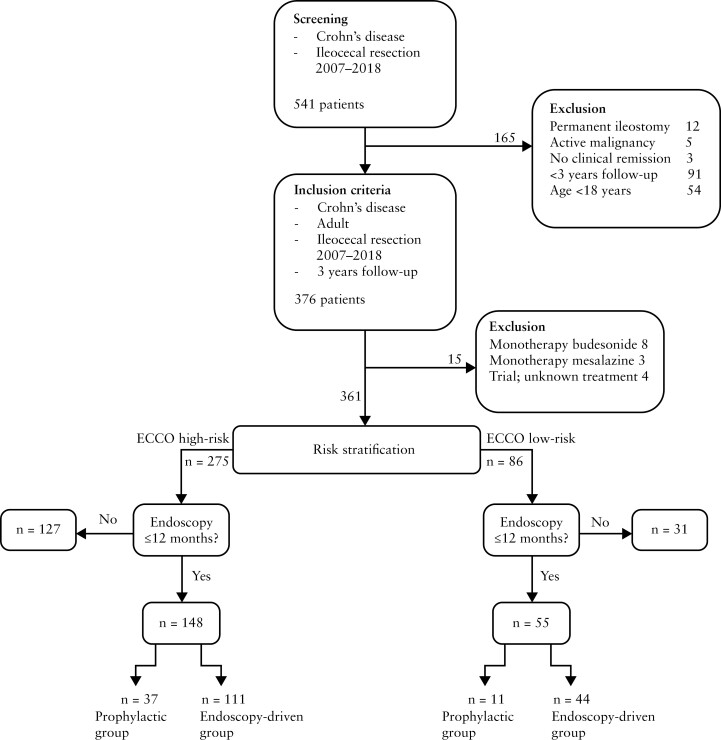
Methods: We retrospectively collected data from 376 consecutive CD patients who underwent an ileocaecal resection with anastomosis between 2007 and 2018 with at least 3 years of follow-up at three sites. Subsequently, high- and low-risk patients categorised by established guidelines, who underwent endoscopy within 12 months postoperatively, were grouped according to a prophylactic- or endoscopy-driven approach and compared for incidence and time till endoscopic and clinical POR.
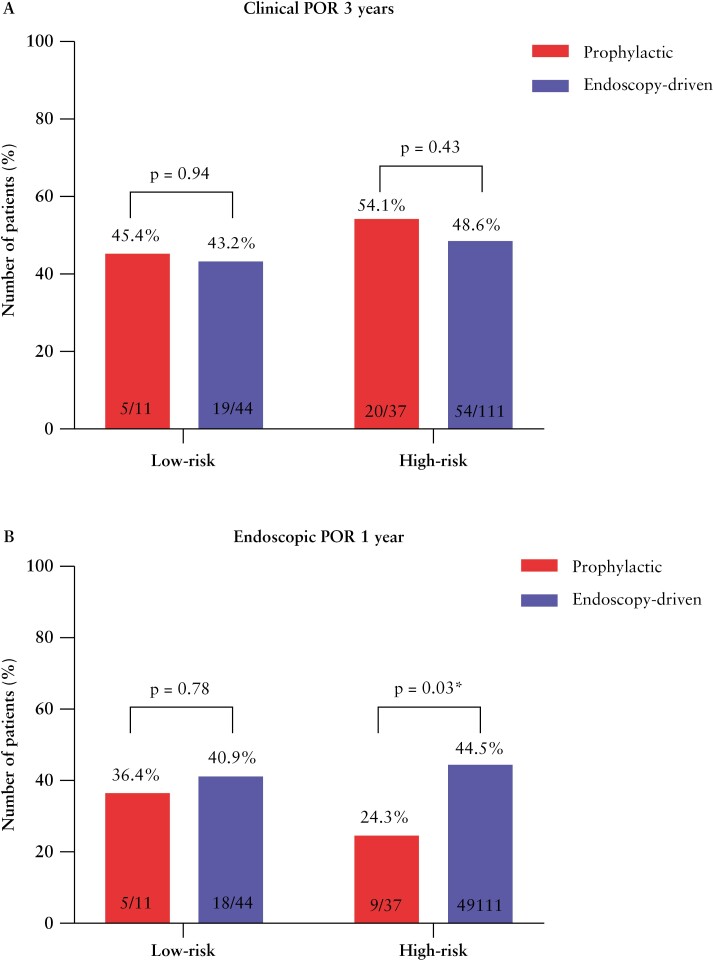
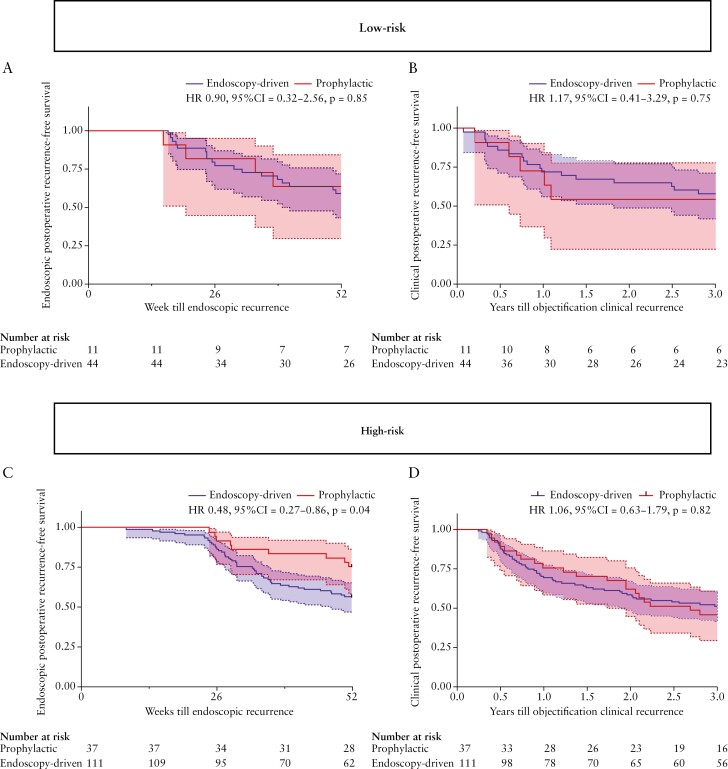
Results: Prophylactic treatment reduced rates of and time till endoscopic POR within 1 year in high-risk (hazard ratio [HR] 0.48, 95% confidence interval [CI] 0.27-0.86, p = 0.04, number needed to treat [NNT] = 5) but not low-risk [HR 0.90, 95% CI 0.32-2.56, p = 0.85] patients. Conversely, no significant differences in clinical POR within 3 years between prophylactic- and endoscopy-driven low-risk [HR 1.17, 95% CI 0.41-3.29, p = 0.75] and high-risk patients were observed [HR 1.06, 95% CI 0.63-1.79, p = 0.82, NNT = 22]. However, a large numerical albeit not statistical significant difference in 3-year clinical POR [28.6% vs. 62.5%, p = 0.11] in a subset of high-risk patients with three or more ECCO-defined risk factors was observed, indicating a cumulative effect of having multiple risk factors.
Conclusion: Our observations favour step-up treatment guided by early endoscopic evaluation with prophylactic treatment reserved for carefully selected high-risk patients, in order to avoid potential overtreatment of a significant number of patients.
Keywords: Inflammatory bowel disease; postoperative recurrence; prevention; risk stratification.
© The Author(s) 2022. Published by Oxford University Press on behalf of European Crohn’s and Colitis Organisation.
Conflict of interest statement
VJ, JS, EW MD, JJ, JB, AM, WL, WB, CB, GD: none to declare. NdB has served as a speaker for AbbVie and MSD and has served as consultant and/or principal investigator for TEVA Pharma BV and Takeda. He has received [unrestricted] research grant from Dr Falk, TEVA Pharma BV, MLDS, and Takeda, all outside the submitted work.
Figures
Comment in
-
The Tortoise (Endoscopy-Driven Treatment) and the Hare (Prophylactic Treatment): Who Wins the Race to Beat Post-Operative Recurrence of Crohn's Disease?J Crohns Colitis. 2023 Apr 3;17(3):309-310. doi: 10.1093/ecco-jcc/jjac165. J Crohns Colitis. 2023. PMID: 36394429 No abstract available.
References
-
- Gionchetti P, Dignass A, Danese S, et al. . Third European Evidence-based consensus on the diagnosis and management of Crohn’s disease 2016. Part 2: surgical management and special situations. J Crohns Colitis 2017;11:135–49. - PubMed
-
- Dragoni G, Ding N, Gecse KB, et al. . The prevention and management of Crohn’s disease postoperative recurrence: results from the Y-ECCO/ClinCom 2019 Survey. Eur J Gastroenterol Hepatol 2020;32:1062–6. - PubMed
-
- Nguyen GC, LoftusHirano EVI, Falck-Ytter Y, Singh S, Sultan S.. American Gastroenterological Association Institute Guideline on the Management of Crohn’s Disease After Surgical Resection. Gastroenterology 2017;152:271–5. - PubMed
MeSH terms
LinkOut - more resources
Full Text Sources
Medical
