

Artificial Intelligence for Contrast-Free MRI: Scar Assessment in Myocardial Infarction Using Deep Learning-Based Virtual Native Enhancement
- PMID: 36124774
- PMCID: PMC9662825
- DOI: 10.1161/CIRCULATIONAHA.122.060137
Artificial Intelligence for Contrast-Free MRI: Scar Assessment in Myocardial Infarction Using Deep Learning-Based Virtual Native Enhancement
Abstract
Background: Myocardial scars are assessed noninvasively using cardiovascular magnetic resonance late gadolinium enhancement (LGE) as an imaging gold standard. A contrast-free approach would provide many advantages, including a faster and cheaper scan without contrast-associated problems.
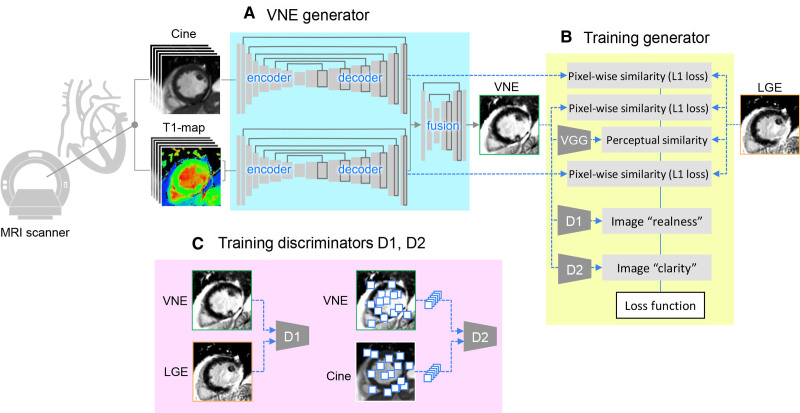
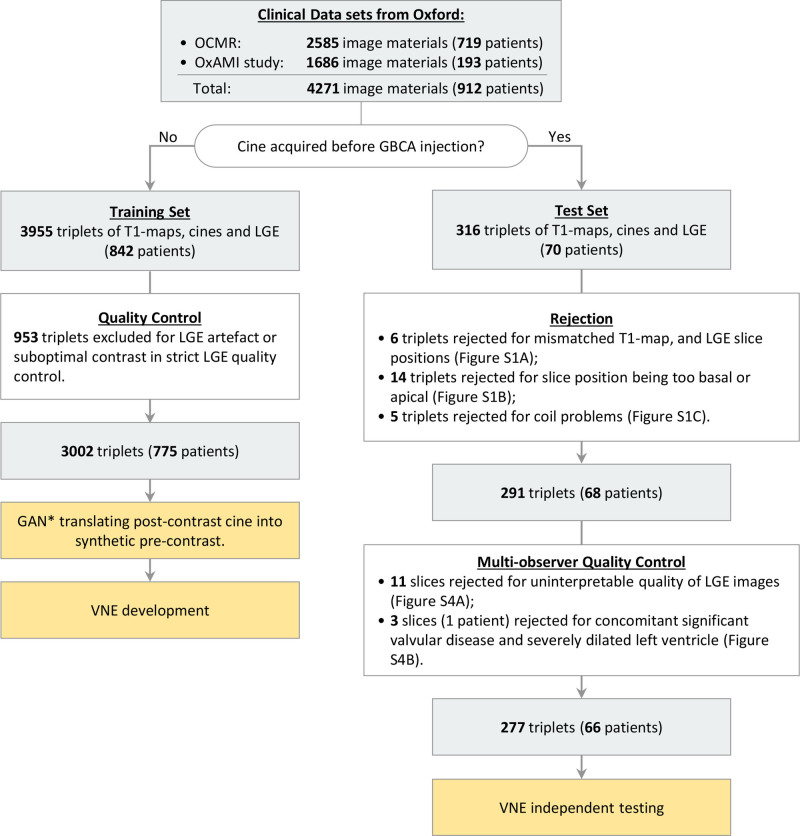
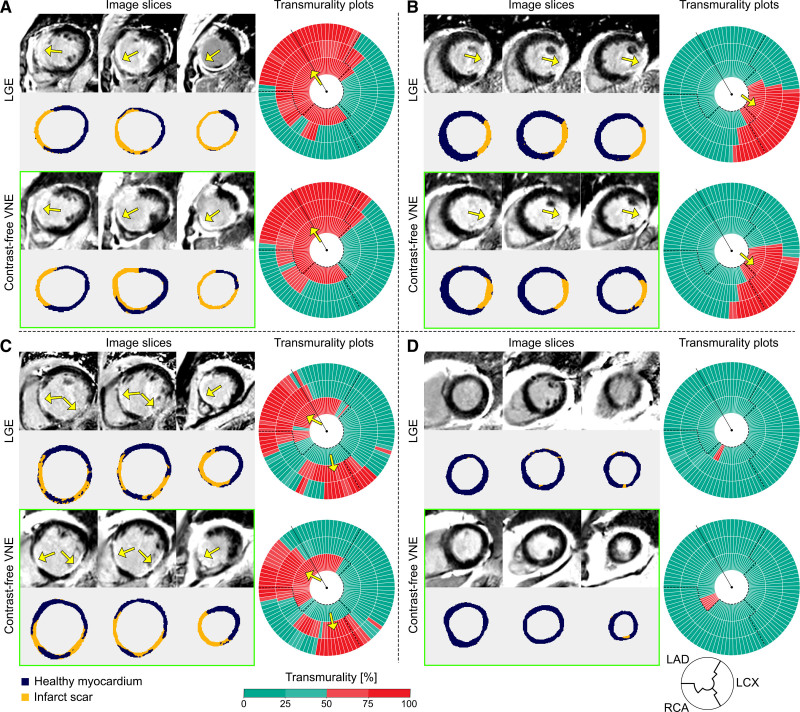
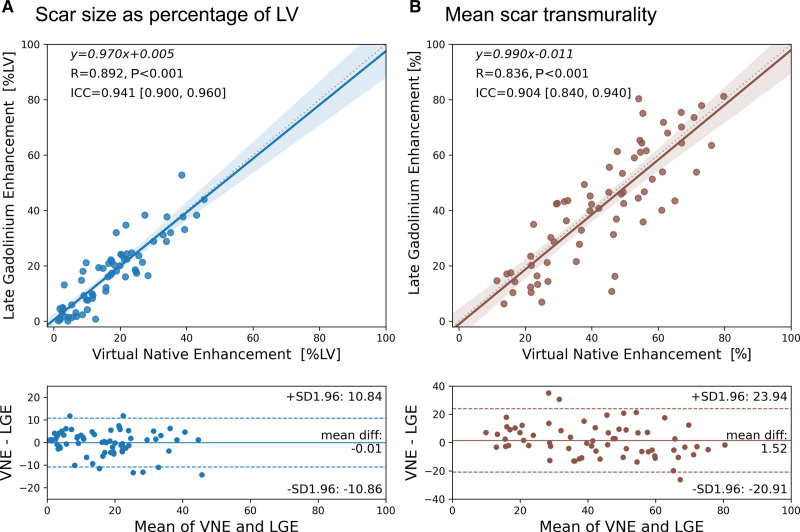
Methods: Virtual native enhancement (VNE) is a novel technology that can produce virtual LGE-like images without the need for contrast. VNE combines cine imaging and native T1 maps to produce LGE-like images using artificial intelligence. VNE was developed for patients with previous myocardial infarction from 4271 data sets (912 patients); each data set comprises slice position-matched cine, T1 maps, and LGE images. After quality control, 3002 data sets (775 patients) were used for development and 291 data sets (68 patients) for testing. The VNE generator was trained using generative adversarial networks, using 2 adversarial discriminators to improve the image quality. The left ventricle was contoured semiautomatically. Myocardial scar volume was quantified using the full width at half maximum method. Scar transmurality was measured using the centerline chord method and visualized on bull's-eye plots. Lesion quantification by VNE and LGE was compared using linear regression, Pearson correlation (R), and intraclass correlation coefficients. Proof-of-principle histopathologic comparison of VNE in a porcine model of myocardial infarction also was performed.
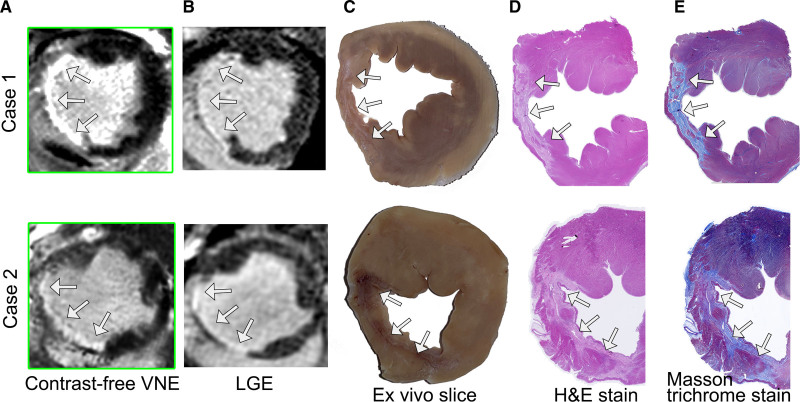
Results: VNE provided significantly better image quality than LGE on blinded analysis by 5 independent operators on 291 data sets (all P<0.001). VNE correlated strongly with LGE in quantifying scar size (R, 0.89; intraclass correlation coefficient, 0.94) and transmurality (R, 0.84; intraclass correlation coefficient, 0.90) in 66 patients (277 test data sets). Two cardiovascular magnetic resonance experts reviewed all test image slices and reported an overall accuracy of 84% for VNE in detecting scars when compared with LGE, with specificity of 100% and sensitivity of 77%. VNE also showed excellent visuospatial agreement with histopathology in 2 cases of a porcine model of myocardial infarction.
Conclusions: VNE demonstrated high agreement with LGE cardiovascular magnetic resonance for myocardial scar assessment in patients with previous myocardial infarction in visuospatial distribution and lesion quantification with superior image quality. VNE is a potentially transformative artificial intelligence-based technology with promise in reducing scan times and costs, increasing clinical throughput, and improving the accessibility of cardiovascular magnetic resonance in the near future.
Keywords: artificial intelligence; cicatrix; magnetic resonance imaging; myocardial infarction.
Figures
Comment in
-
Artificial Intelligence to Extract Endogenous Tissue Characteristics: Has the Future Free From Gadolinium Contrast Arrived?Circulation. 2022 Nov 15;146(20):1504-1506. doi: 10.1161/CIRCULATIONAHA.122.062147. Epub 2022 Nov 14. Circulation. 2022. PMID: 36374971 No abstract available.
References
-
- Roth GA, Mensah GA, Johnson CO, Addolorato G, Ammirati E, Baddour LM, Barengo NC, Beaton AZ, Benjamin EJ, Benziger CP, et al. Global burden of cardiovascular diseases and risk factors, 1990–2019: update from the GBD 2019 study. J Am Coll Cardiol. 2020;76:2982–3021. doi: 10.1016/j.jacc.2020.11.010 - PMC - PubMed
-
- Roes SD, Kelle S, Kaandorp TAM, Kokocinski T, Poldermans D, Lamb HJ, Boersma E, van der Wall EE, Fleck E, de Roos A, et al. Comparison of myocardial infarct size assessed with contrast-enhanced magnetic resonance imaging and left ventricular function and volumes to predict mortality in patients with healed myocardial infarction. Am J Cardiol. 2007;100:930–936. doi: 10.1016/j.amjcard.2007.04.029 - PubMed
-
- Kelle S, Roes SD, Klein C, Kokocinski T, de Roos A, Fleck E, Bax JJ, Nagel E. Prognostic value of myocardial infarct size and contractile reserve using magnetic resonance imaging. J Am Coll Cardiol. 2009;54:1770–1777. doi: 10.1016/j.jacc.2009.07.027 - PubMed
-
- Wagner A, Mahrholdt H, Holly TA, Elliott MD, Regenfus M, Parker M, Klocke FJ, Bonow RO, Kim RJ, Judd RM. Contrast-enhanced MRI and routine single photon emission computed tomography (SPECT) perfusion imaging for detection of subendocardial myocardial infarcts: an imaging study. Lancet. 2003;361:374–379. doi: 10.1016/s0140-6736(03)12389-6 - PubMed
-
- Thiele H, Kappl MJE, Conradi S, Niebauer J, Hambrecht R, Schuler G. Reproducibility of chronic and acute infarct size measurement by delayed enhancement-magnetic resonance imaging. J Am Coll Cardiol. 2006;47:1641–1645. doi: 10.1016/j.jacc.2005.11.065 - PubMed
Publication types
MeSH terms
Substances
Grants and funding
LinkOut - more resources
Full Text Sources
Medical
