

Clinical governance of patients with acute coronary syndromes
- PMID: 36124872
- PMCID: PMC9709629
- DOI: 10.1093/ehjacc/zuac106
Clinical governance of patients with acute coronary syndromes
Erratum in
-
Corrigendum to: Clinical governance of patients with acute coronary syndromes.Eur Heart J Acute Cardiovasc Care. 2023 Feb 9;12(2):138. doi: 10.1093/ehjacc/zuac155. Eur Heart J Acute Cardiovasc Care. 2023. PMID: 36542474 Free PMC article. No abstract available.
Abstract
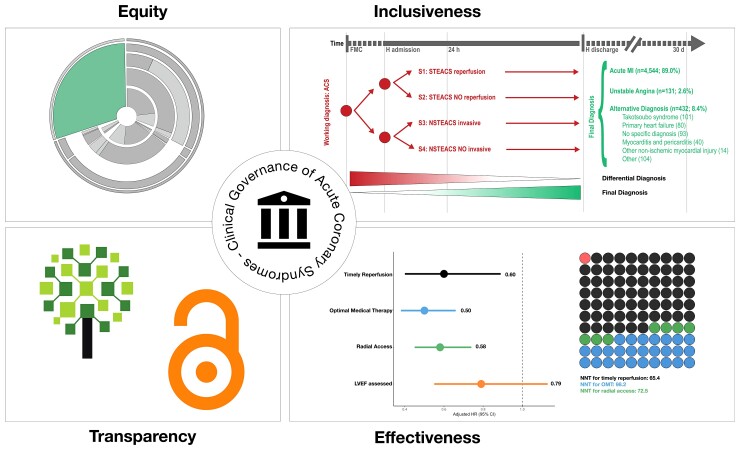
Aims: Using the principles of clinical governance, a patient-centred approach intended to promote holistic quality improvement, we designed a prospective, multicentre study in patients with acute coronary syndrome (ACS). We aimed to verify and quantify consecutive inclusion and describe relative and absolute effects of indicators of quality for diagnosis and therapy.
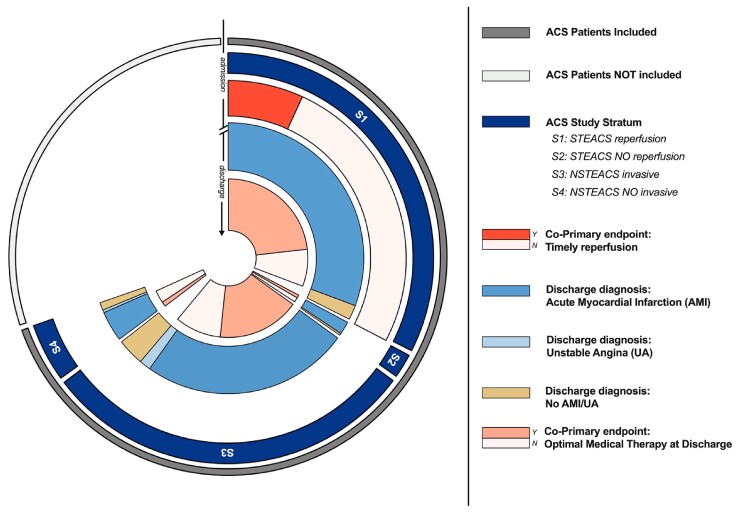
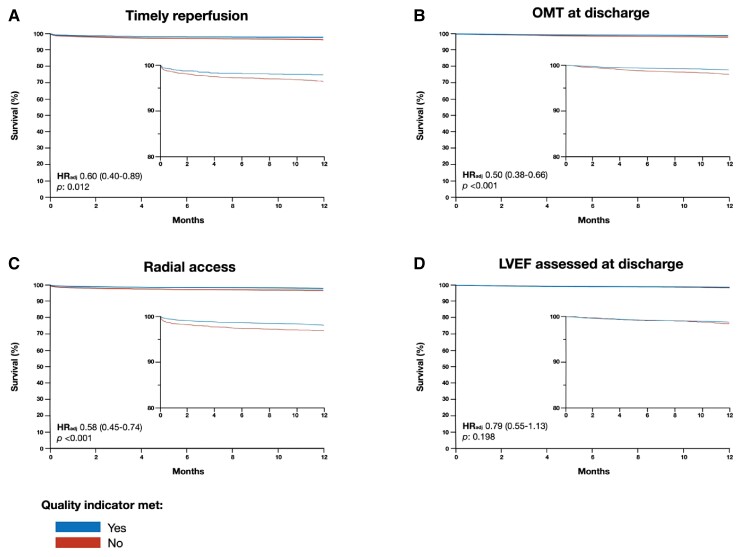
Methods and results: Administrative codes for invasive coronary angiography and acute myocardial infarction were used to estimate the ACS universe. The ratio between the number of patients included and the estimated ACS universe was the consecutive index. Co-primary quality indicators were timely reperfusion in patients admitted with ST-elevation ACS and optimal medical therapy at discharge. Cox-proportional hazard models for 1-year death with admission and discharge-specific covariates quantified relative risk reductions and adjusted number needed to treat (NNT) absolute risk reductions. Hospital codes tested had a 99.5% sensitivity to identify ACS universe. We estimated that 7344 (95% CI: 6852-7867) ACS patients were admitted and 5107 were enrolled-i.e. a consecutive index of 69.6% (95% CI 64.9-74.5%), which varied from 30.7 to 79.2% across sites. Timely reperfusion was achieved in 22.4% (95% CI: 20.7-24.1%) of patients, was associated with an adjusted hazard ratio (HR) for 1-year death of 0.60 (95% CI: 0.40-0.89) and an adjusted NNT of 65 (95% CI: 44-250). Corresponding values for optimal medical therapy were 70.1% (95% CI: 68.7-71.4%), HR of 0.50 (95% CI: 0.38-0.66), and NNT of 98 (95% CI: 79-145).
Conclusion: A comprehensive approach to quality for patients with ACS may promote equitable access of care and inform implementation of health care delivery.
Registration: ClinicalTrials.Gov ID NCT04255537.
Keywords: acute coronary syndromes; clinical governance; quality improvement.
© The Author(s) 2022. Published by Oxford University Press on behalf of the European Society of Cardiology.
Conflict of interest statement
Conflicts of interest: S.L. reports grants and personal fees from Astra Zeneca, personal fees from Daiichi Sankyo, personal fees from Bayer, personal fees from Pfizer/BMS, personal fees from ICON, personal fees from Chiesi, personal fees from Novonordisk, all outside the submitted work. C.M. has nothing to disclose. G.Carrara reports personal fee from Advice Pharma during the conduct of the study. G.Casella has nothing to disclose. D.G. reports he has participated in advisory boards for Amgen and for Sanofi, outside the submitted work. M.G., A.R., L.T., M.P., F.O., M.G., L.G., L.S.C., Dr. S.D.S., and A.A. have nothing to disclose. G.M.D.F. serves as member of the steering committee for Amgen and consultant for UCB. L.O.V. reports personal fees from Eli Lilly; personal fees from Daiichi Sankyo, personal fees from AstraZeneca; personal fees from Menarini; personal fees from Bayer; personal fees from Pfizer; personal fees from BMS; personal fees from Boehringer Ingelheim, all outside the submitted work. Prof. Campo reports grants from SMT; grants from Siemens; Grants from MEDIS; grants from Boston Scientific, grants from GE Healthcare, all outside the submitted work.
Figures
References
-
- Hunter DJ. The complementarity of public health and medicine - achieving “the highest attainable standard of health”. N Engl J Med 2021;385:481–484. - PubMed
-
- Leonardi S, Montalto C, Casella G, Grosseto D, Repetto A, Portolan M, Fortuni F, Ottani F, Galvani M, Cardelli LS, De Servi S, Rubboli A, De Ferrari GM, Oltrona Visconti L, Campo G.. Clinical governance programme in patients with acute coronary syndrome: design and methodology of a quality improvement initiative. Open Heart 2020;7:e001415. - PMC - PubMed
-
- Peterson ED, Roe MT, Chen AY, Fonarow GC, Lytle BL, Cannon CP, Rumsfeld JS.. The NCDR action registry-GWTG: transforming contemporary acute myocardial infarction clinical care. Heart 2010;96:1798–1802. - PubMed
-
- Grambsch PM, Therneau TM. Proportional hazards tests and diagnostics based on weighted residuals. Biometrika 1994;81:515–526.
Publication types
MeSH terms
Associated data
Grants and funding
LinkOut - more resources
Full Text Sources
Medical
