

Acute Kidney Injury after High-Flow Regional Cerebral Perfusion in Neonatal and Infant Aortic Arch Repair
- PMID: 36124960
- PMCID: PMC9950871
- DOI: 10.1093/icvts/ivac247
Acute Kidney Injury after High-Flow Regional Cerebral Perfusion in Neonatal and Infant Aortic Arch Repair
Abstract
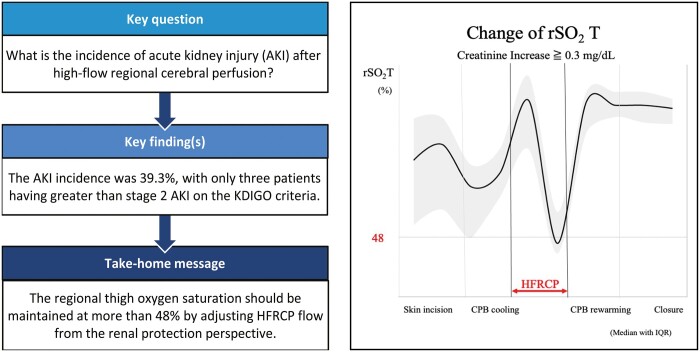
Objectives: We applied high-flow regional cerebral perfusion (HFRCP) for aortic arch reconstruction in neonates and infants by monitoring regional oxygen saturation of the thigh (rSO2T) using near-infrared spectroscopy to maintain peripheral perfusion. This study was designed to investigate the optimal perfusion flow of HFRCP for renal protection.
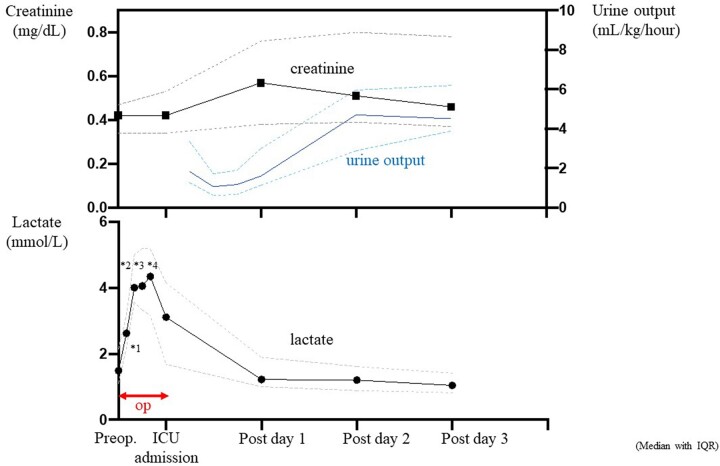
Methods: From 2009 to 2021, 28 consecutive neonates and infants who underwent aortic arch reconstruction with HFRCP were enrolled. The median age of the patients was 27 days; the median body weight was 3.0 kg. In HFRCP, perfusion flow was targeted at approximately 80-100 mL/kg/min and then lowered corresponding to brain rSO2 levels and blood gas data. Isosorbide dinitrate and chlorpromazine were administered to enhance peripheral perfusion flow. Regional oxygen saturation of the forehead and thighs were monitored. The stage of acute kidney injury (AKI) was classified based on the Kidney Disease Improving Global Outcomes criteria.
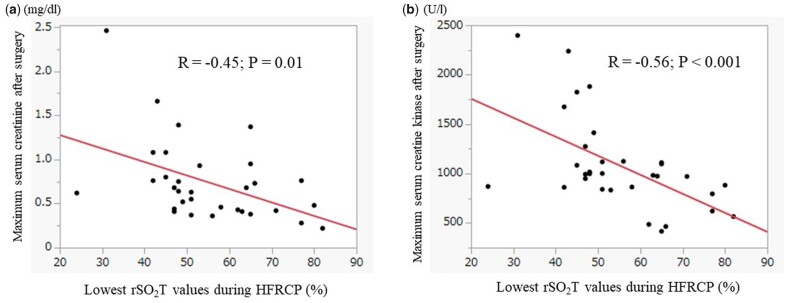
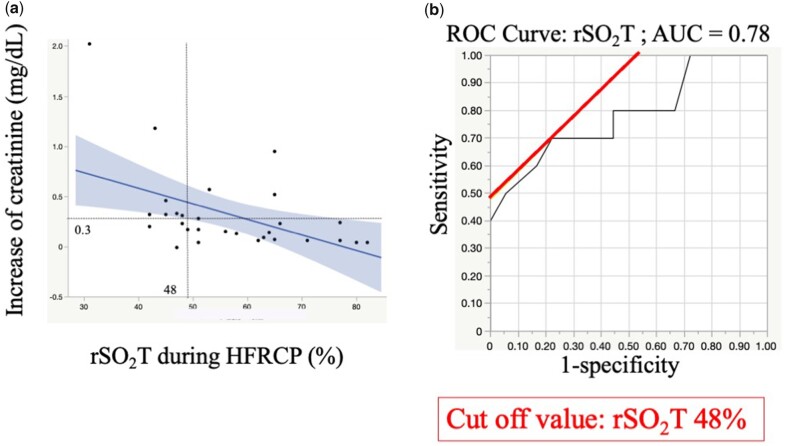
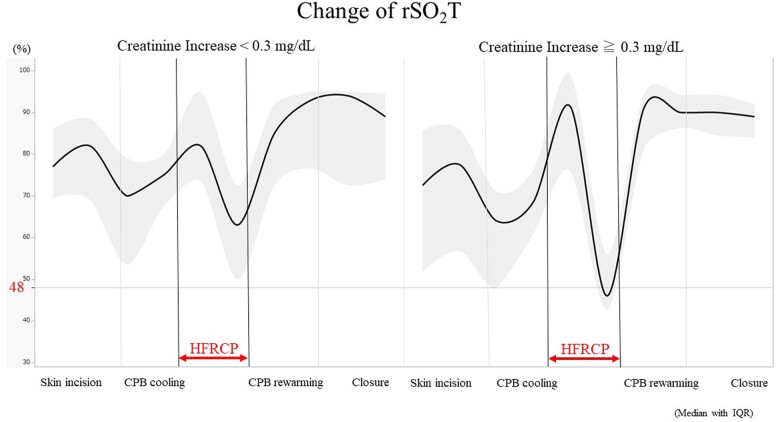
Results: No patients had neurological events and peritoneal dialysis after surgery. The incidence of AKI was 39.3% with only three patients having greater than stage 2 AKI. The maximum postoperative serum creatinine concentration was negatively associated with the lowest rSO2T during HFRCP. The rSO2T during HFRCP was a predictive factor for postoperative creatinine increase of ≧0.3 mg/dL. The area under receiver operating characteristic curve was 0.78 with the cutoff value of 48% for rSO2T.
Conclusions: The rSO2T during HFRCP is a potential predictor of postoperative renal function. To prevent AKI, the rSO2T should be preserved more than 48% by increasing HFRCP flow.
Keywords: aortic arch repairs; congenital heart surgery; infants; neonates.
© The Author(s) 2022. Published by Oxford University Press on behalf of the European Association for Cardio-Thoracic Surgery.
Figures

Comment in
-
Regional cerebral perfusion during arch repair in infants: there is always room for improvement.Interdiscip Cardiovasc Thorac Surg. 2023 Feb 6;36(2):ivad008. doi: 10.1093/icvts/ivad008. Interdiscip Cardiovasc Thorac Surg. 2023. PMID: 36847680 Free PMC article. No abstract available.
References
-
- Lodge AJ, Andersen ND, Turek JW.. Recent advances in congenital heart surgery: alternative perfusion strategies for infant aortic arch repair. Curr Cardiol Rep 2019;21:13. - PubMed
-
- Wypij D, Newburger JW, Rappaport LA, duPlessis AJ, Jonas RA, Wernovsky G. et al. The effect of duration of deep hypothermic circulatory arrest in infant heart surgery on late neurodevelopment: the Boston Circulatory Arrest Trial. J Thorac Cardiovasc Surg 2003;126:1397–403. - PubMed
-
- Miyaji K, Miyamoto T, Kohira S, Itatani K, Tomoyasu T, Inoue N. et al. Regional high-flow cerebral perfusion improves both cerebral and somatic tissue oxygenation in aortic arch repair. Ann Thorac Surg 2010;90:593–9. - PubMed
LinkOut - more resources
Full Text Sources
