

A systematic approach to CT evaluation of non-arthritic hip pain
- PMID: 36125004
- PMCID: PMC9624481
- DOI: 10.1530/EOR-22-0051
A systematic approach to CT evaluation of non-arthritic hip pain
Abstract
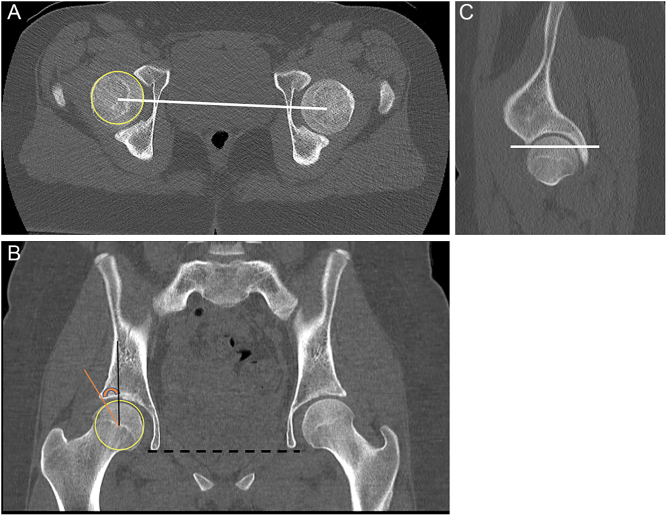
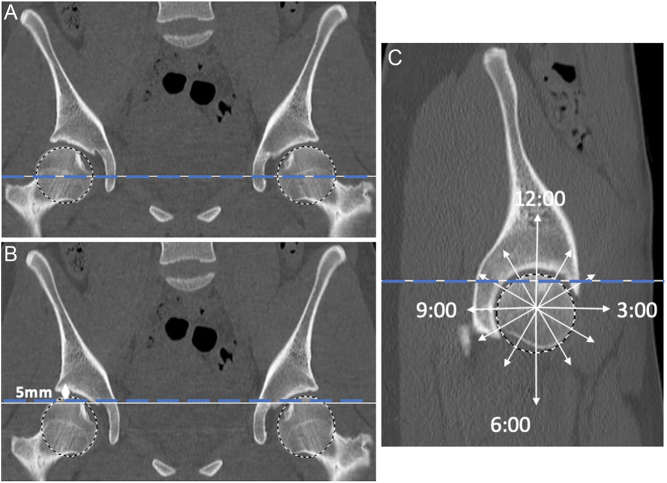
Bone morphology has been increasingly recognized as a significant variable in the evaluation of non-arthritic hip pain in young adults. Increased availability and use of multidetector CT in this patient population has contributed to better characterization of the osseous structures compared to traditional radiographs. Femoral and acetabular version, sites of impingement, acetabular coverage, femoral head-neck morphology, and other structural abnormalities are increasingly identified with the use of CT scan. In this review, a standard CT imaging technique and protocol is discussed, along with a systematic approach for evaluating pelvic CT imaging in patients with non-arthritic hip pain.
Keywords: computed tomography; femoroacetabular impingement; hip/thigh/pelvis.
Conflict of interest statement
The authors declare that there is no conflict of interest that could be perceived as prejudicing the impartiality of the research reported.
Figures









Similar articles
-
Revisiting the Anteroinferior Iliac Spine: Is the Subspine Pathologic? A Clinical and Radiographic Evaluation.Clin Orthop Relat Res. 2018 Jul;476(7):1494-1502. doi: 10.1097/01.blo.0000533626.25502.e1. Clin Orthop Relat Res. 2018. PMID: 29794857 Free PMC article.
-
Femoral Morphology in the Dysplastic Hip: Three-dimensional Characterizations With CT.Clin Orthop Relat Res. 2017 Apr;475(4):1045-1054. doi: 10.1007/s11999-016-5119-2. Clin Orthop Relat Res. 2017. PMID: 27752989 Free PMC article.
-
Location of Intra- and Extra-articular Hip Impingement Is Different in Patients With Pincer-Type and Mixed-Type Femoroacetabular Impingement Due to Acetabular Retroversion or Protrusio Acetabuli on 3D CT-Based Impingement Simulation.Am J Sports Med. 2020 Mar;48(3):661-672. doi: 10.1177/0363546519897273. Epub 2020 Jan 21. Am J Sports Med. 2020. PMID: 31961701
-
Ultrasound Evaluation of the Hip.Curr Rev Musculoskelet Med. 2024 Dec;17(12):548-558. doi: 10.1007/s12178-024-09929-4. Epub 2024 Oct 31. Curr Rev Musculoskelet Med. 2024. PMID: 39477906 Free PMC article. Review.
-
[Femoroacetabular impingement related to Legg-Calvé-Perthes disease].Srp Arh Celok Lek. 2011 Nov-Dec;139(11-12):834-7. doi: 10.2298/sarh1112834v. Srp Arh Celok Lek. 2011. PMID: 22338487 Review. Serbian.
References
-
- Beck M, Kalhor M, Leunig M, Ganz R. Hip morphology influences the pattern of damage to the acetabular cartilage: femoroacetabular impingement as a cause of early osteoarthritis of the hip. Journal of Bone and Joint Surgery: British Volume 2005871012–1018. (10.1302/0301-620X.87B7.15203) - DOI - PubMed
Publication types
LinkOut - more resources
Full Text Sources
