

The Canadian Mother-Child Cohort Active Surveillance Initiative (CAMCCO): Comparisons between Quebec, Manitoba, Saskatchewan, and Alberta
- PMID: 36126025
- PMCID: PMC9488808
- DOI: 10.1371/journal.pone.0274355
The Canadian Mother-Child Cohort Active Surveillance Initiative (CAMCCO): Comparisons between Quebec, Manitoba, Saskatchewan, and Alberta
Abstract
Background: Given that pregnant women taking medications are excluded from clinical trials, real-world evidence is essential. We aimed to build a Canadian Mother-Child Cohort Active Surveillance Initiative (CAMCCO) and compare frequency of prematurity, low-birth-weight (LBW), major malformations, multiplicity, and gestational medication use across four provinces.
Methods: CAMCCO is a collaborative research infrastructure that uses real-world data from large provincial health care databases in Canada; developed with standardized methods to similarly construct population-based pregnancy/child cohorts with longitudinal follow-up by linking administrative/hospital/birth databases. CAMCCO also includes a common repository to i) share algorithms and case definitions based on diagnostic and procedural codes for research/training purpose, and ii) download aggregate data relevant to primary care providers, researchers, and decision makers. For this study, data from Quebec (1998-2015), Manitoba (1995-2019), Saskatchewan (1996-2020), and Alberta (2005-2018) are compared (Chi-square tests, p-values), and trends are calculated using Cochran-Armitage trend tests.
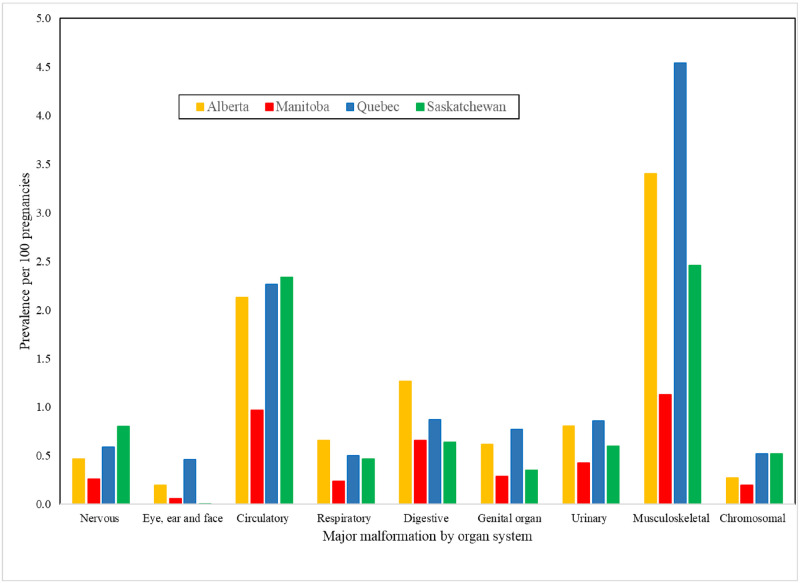
Results: Almost two-thirds (61%) of women took medications during pregnancy, mostly antibiotics (26%), asthma drugs (8%), and antidepressants (4%). Differences in the prevalence of prematurity (5.9-6.8%), LBW (4.0-5.2%), and multiplicity (1.0-2.5%) were statistically significant between provinces (p<0.001). Frequency of major malformations increased over time in Quebec (7-11%; p<0.001), Saskatchewan (5-11%; p<0.001), and Alberta (from 7-8%; p<0.001), and decreased in Manitoba (5-3%; p<0.001). Cardiovascular and musculoskeletal malformations were the most prevalent.
Interpretation: Medications are often used among Canadian pregnancies but adverse pregnancy outcomes vary across provinces. Digitized health data may help researchers and care providers understand the risk-benefit ratios related to gestational medication use, as well as province-specific trends.
Conflict of interest statement
The authors have declared that no competing interests exist.
Figures



References
-
- Margulis AV, Abou-Ali A, Strazzeri MM, Ding Y, Kuyateh F, Frimpong EY, et al.. Use of selective serotonin reuptake inhibitors in pregnancy and cardiac malformations: a propensity-score matched cohort in CPRD. Pharmacoepidemiol Drug Saf. 2013. Sep;22(9):942–51. doi: 10.1002/pds.3462 Epub 2013 Jun 3. . - DOI - PubMed
-
- Bearak J, Popinchalk A, Ganatra B, Moller AB, Tunçalp Ö, Beavin C, et al.. Unintended pregnancy and abortion by income, region, and the legal status of abortion: estimates from a comprehensive model for 1990–2019. Lancet Glob Health. 2020. Sep;8(9):e1152–e1161. doi: 10.1016/S2214-109X(20)30315-6 Epub 2020 Jul 22. . - DOI - PubMed
Publication types
MeSH terms
Grants and funding
LinkOut - more resources
Full Text Sources
