

Identification of immune and stromal cell infiltration-related gene signature for prognosis prediction in acute lymphoblastic leukemia
- PMID: 36126190
- PMCID: PMC9550239
- DOI: 10.18632/aging.204292
Identification of immune and stromal cell infiltration-related gene signature for prognosis prediction in acute lymphoblastic leukemia
Abstract
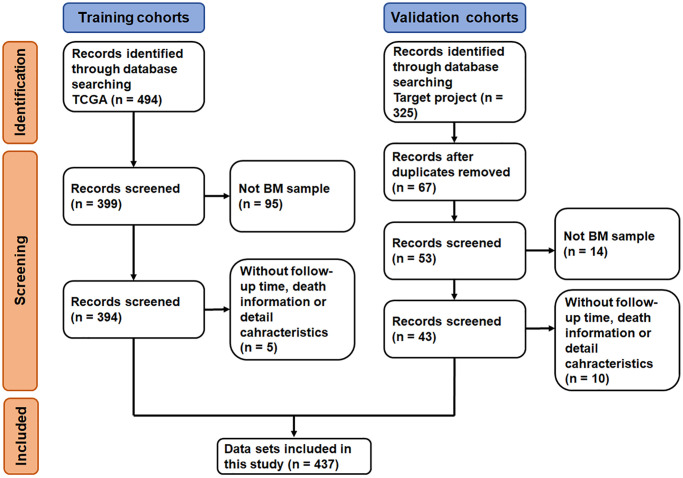
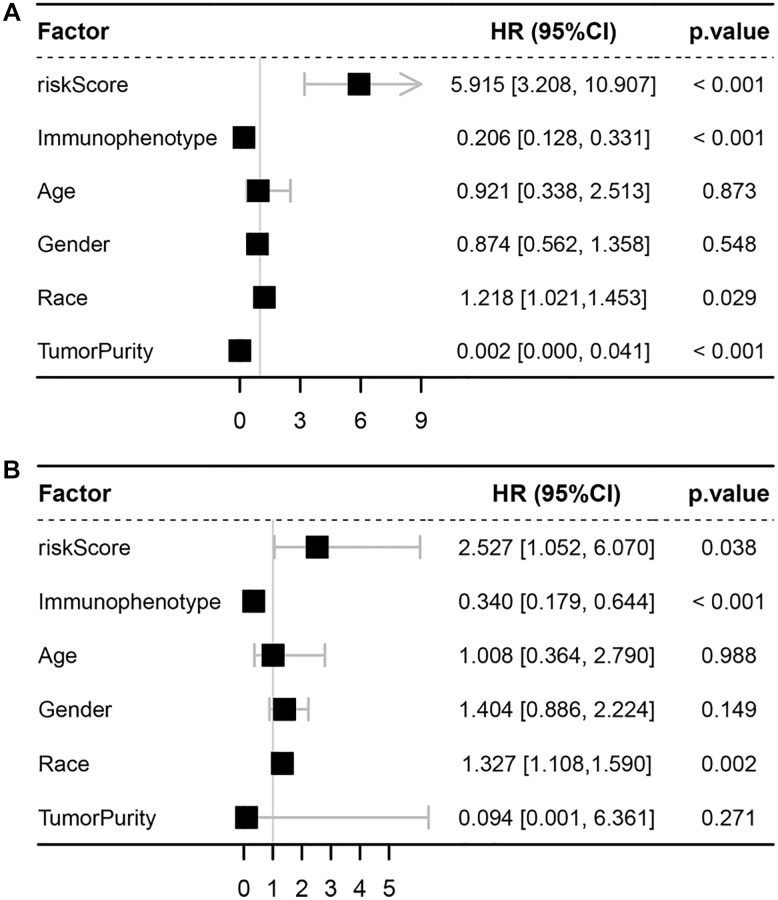
Acute lymphoblastic leukemia (ALL) is a common and life-threatening hematologic malignancy, its occurrence and progression are closely related to immune/stromal cell infiltration in the bone marrow (BM) microenvironment. However, no studies have described an immune/stromal cell infiltration-related gene (ISCIRG)-based prognostic signature for ALL. A total of 444 patients involving 437 bulk and 7 single-cell RNA-seq datasets were included in this study. Eligible datasets were searched and reviewed from the database of TCGA, TARGET project and GEO. Then an integrated bioinformatics analysis was performed to select optimal prognosis-related genes from ISCIRGs, construct a nomogram model for predicting prognosis, and assess the predictive power. After LASSO and multivariate Cox regression analyses, a seven ISCIRGs-based signature was proved to be able to significantly stratify patients into high- and low-risk groups in terms of OS. The seven genes were confirmed that directly related to the composition and status of immune/stromal cells in BM microenvironment by analyzing bulk and single-cell RNA-seq datasets. The calibration plot showed that the predicted results of the nomogram were consistent with the actual observation results of training/validation cohort. This study offers a reference for future research regarding the role of ISCIRGs in ALL and the clinical care of patients.
Keywords: acute lymphoblastic leukemia; bioinformatics; bone marrow microenvironment; immune cell infiltration; overall survival.
Conflict of interest statement
Figures









References
Publication types
MeSH terms
LinkOut - more resources
Full Text Sources
Other Literature Sources
