

Evaluation of a New CT-Guided Robotic System for Percutaneous Needle Insertion for Thermal Ablation of Liver Tumors: A Prospective Pilot Study
- PMID: 36127519
- PMCID: PMC9626422
- DOI: 10.1007/s00270-022-03267-z
Evaluation of a New CT-Guided Robotic System for Percutaneous Needle Insertion for Thermal Ablation of Liver Tumors: A Prospective Pilot Study
Abstract
Purpose: To assess the feasibility and safety of a robotic system for percutaneous needle insertion during thermal ablation of liver tumors.
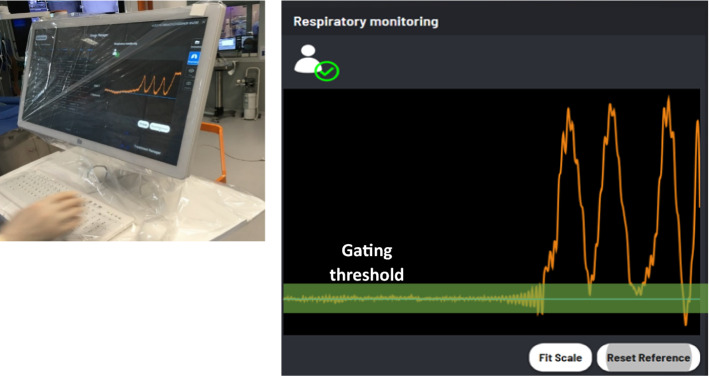
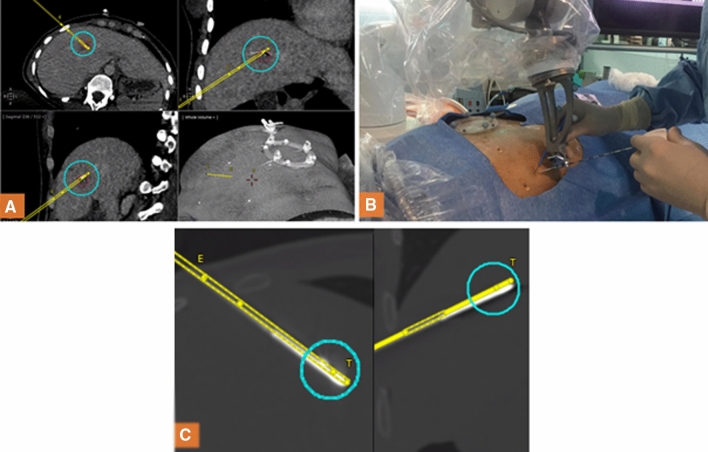
Materials and methods: This study analyzed the CT-guided percutaneous needle insertion using the EPIONE robotic device (Quantum Surgical, Montpellier, France) for radiofrequency or microwave liver ablation. The main criteria of the study were feasibility (possibility to perform the thermal ablation after needle insertion), the number of needle adjustments (reiteration of robotically assisted needle insertion when initial needle positioning is considered insufficient to perform ablation), and robotic-guided procedure safety (complications related to the needle insertion). Patients were followed up at 6 months post-intervention to assess local tumor control.
Results: Twenty-one patients with 24 tumors, including 6 HCC and 18 metastases measuring 15.6 ± 7.2 mm, were enrolled. One patient (with one tumor) was excluded for protocol deviation. Robotic assisted thermal ablation was feasible for 22/23 lesions (95.7%) and 19/20 patients (95.0%), as validated by a data safety monitoring Board (95% CI [76.39%; 99.11%]) for the per-protocol population. The mean number of needle adjustments per tumor treated was 0.4 (SD: 0.7), with 70.8% of tumors requiring no adjustment. No adverse events were depicted. Rate of local tumor control was 83.3% for patients and 85.7% for tumors, at 6 months.
Conclusion: This bicentric first-in-human pilot study suggests both feasibility and safety of a stereotactic CT-guided EPIONE device for the percutaneous needle insertion during liver tumor thermal ablation.
Keywords: Computed tomography; Liver cancer; Needle navigation; Robotic navigation; Thermal ablation.
© 2022. The Author(s).
Conflict of interest statement
The authors of this manuscript declare relationships with the following companies: Thierry de Baère is consultant for and receive research grant from Quantum Surgical, consultant and speaker for Boston Scientific, GE Healthcare, AstraZeneca and Boris Guiu is consultant for Quantum Surgical, Boston Scientific, Canon Medical, Roche, Ipsen, Terumo and received research grant from his work.
Figures



References
MeSH terms
LinkOut - more resources
Full Text Sources
Medical
