

COVID's collateral damage: likelihood of measles resurgence in the United States
- PMID: 36127637
- PMCID: PMC9487857
- DOI: 10.1186/s12879-022-07703-w
COVID's collateral damage: likelihood of measles resurgence in the United States
Abstract
Background: Lockdowns imposed throughout the US to control the COVID-19 pandemic led to a decline in all routine immunizations rates, including the MMR (measles, mumps, rubella) vaccine. It is feared that post-lockdown, these reduced MMR rates will lead to a resurgence of measles.
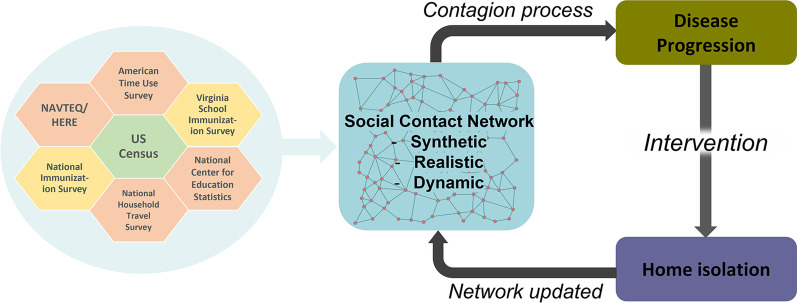
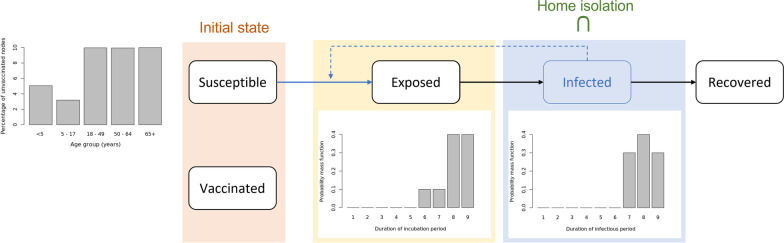
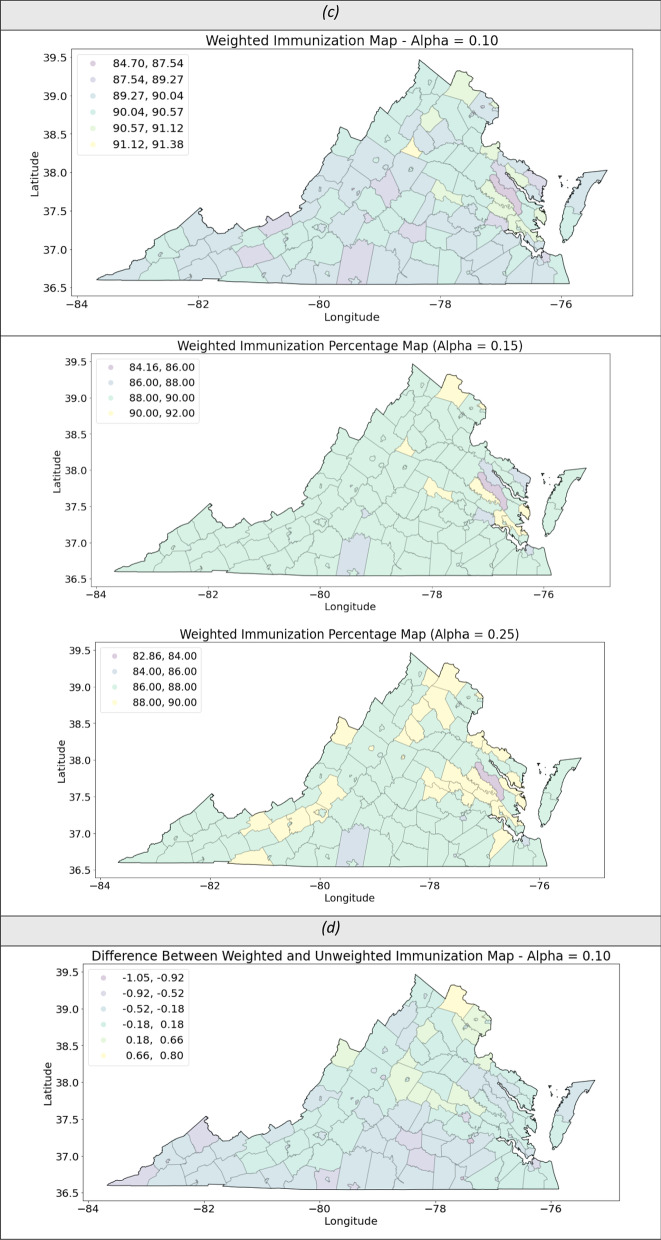
Methods: To measure the potential impact of reduced MMR vaccination rates on measles outbreak, this research examines several counterfactual scenarios in pre-COVID-19 and post-COVID-19 era. An agent-based modeling framework is used to simulate the spread of measles on a synthetic yet realistic social network of Virginia. The change in vulnerability of various communities to measles due to reduced MMR rate is analyzed.
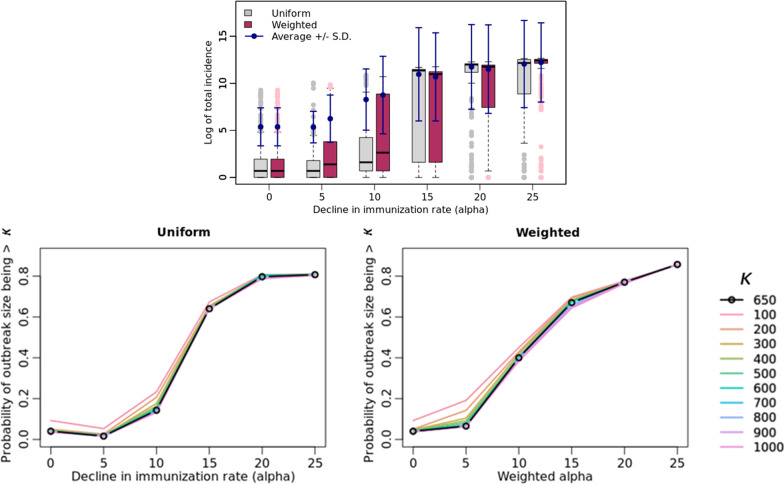
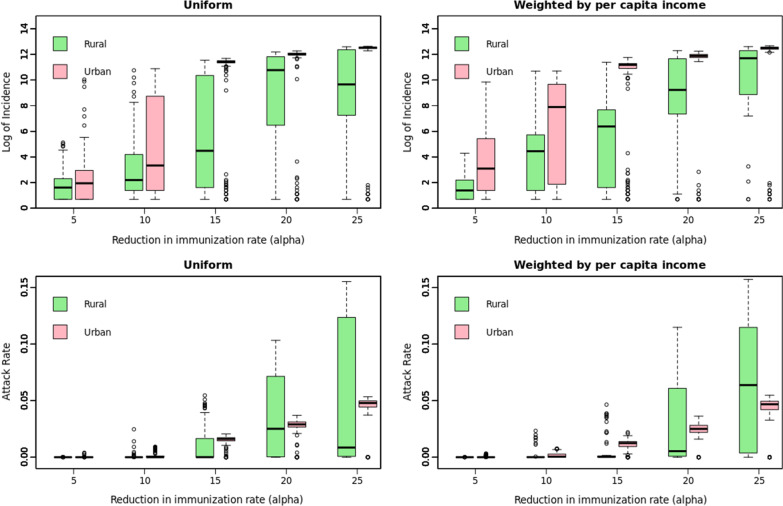
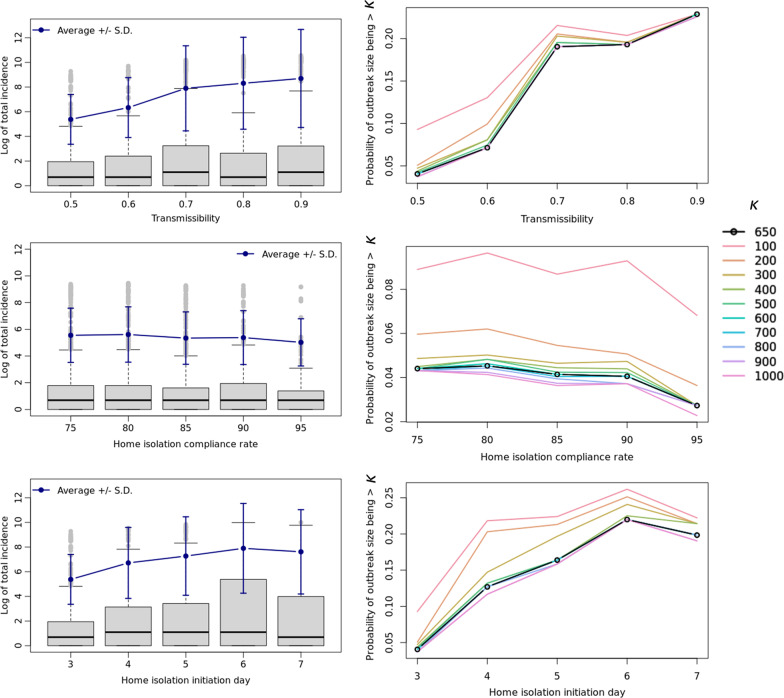
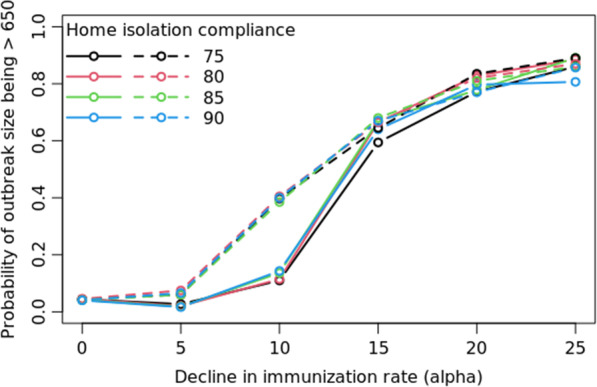
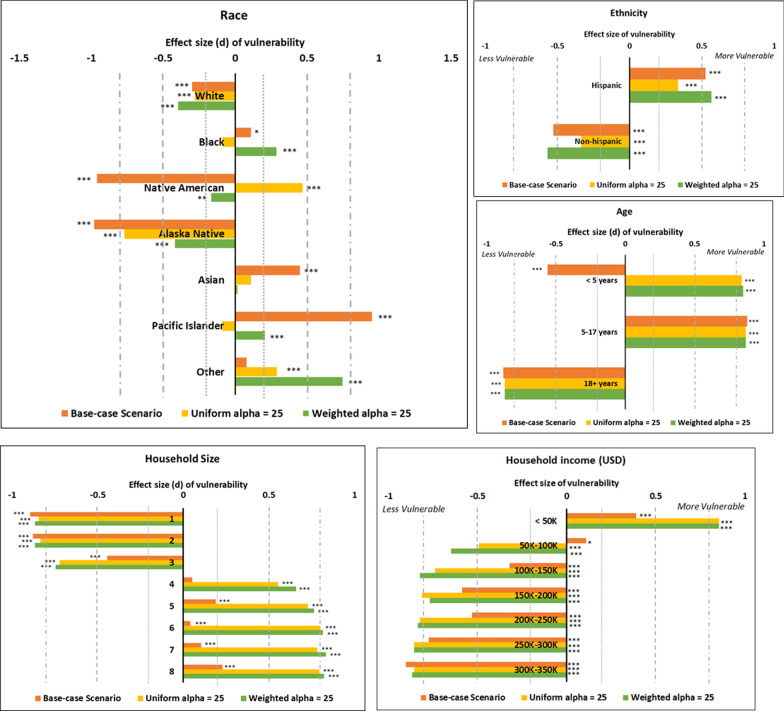
Results: Results show that a decrease in vaccination rate [Formula: see text] has a highly non-linear effect on the number of measles cases and this effect grows exponentially beyond a threshold [Formula: see text]. At low vaccination rates, faster isolation of cases and higher compliance to home-isolation are not enough to control the outbreak. The overall impact on urban and rural counties is proportional to their population size but the younger children, African Americans and American Indians are disproportionately infected and hence are more vulnerable to the reduction in the vaccination rate.
Conclusions: At low vaccination rates, broader interventions are needed to control the outbreak. Identifying the cause of the decline in vaccination rates (e.g., low income) can help design targeted interventions which can dampen the disproportional impact on more vulnerable populations and reduce disparities in health. Per capita burden of the potential measles resurgence is equivalent in the rural and the urban communities and hence proportionally equitable public health resources should be allocated to rural regions.
Keywords: Agent-based model; Health equity; Home isolation; MMR vaccination; NIS; Network epidemiology; Social network; Vulnerable populations.
© 2022. The Author(s).
Conflict of interest statement
The authors declare that they have no competing interests.
Figures

References
-
- Santoli JM. Effects of the COVID-19 pandemic on routine pediatric vaccine ordering and administration—United States, 2020. MMWR. Morbidity and mortality weekly report. 2020;69. - PubMed
MeSH terms
Substances
Grants and funding
LinkOut - more resources
Full Text Sources
Medical
