

Salvianolic acid A alleviates lipopolysaccharide-induced disseminated intravascular coagulation by inhibiting complement activation
- PMID: 36127691
- PMCID: PMC9487091
- DOI: 10.1186/s12906-022-03720-z
Salvianolic acid A alleviates lipopolysaccharide-induced disseminated intravascular coagulation by inhibiting complement activation
Abstract
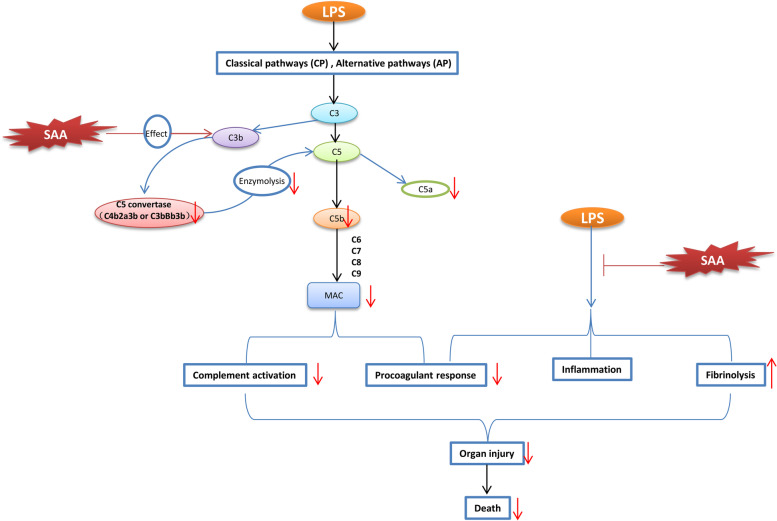
Introduction: Disseminated intravascular coagulation (DIC) is a syndrome characterized by coagulopathy, microthrombus, and multiple organ failure. The complement system in DIC is overactivated, and the functions of complement and coagulation pathways are closely related. Our previous screening revealed that salvianolic acid A (SAA) has anti-complement activity. The hyper-activated complement system was involved in the lipopolysaccharide (LPS) induced DIC in rats. The effects of SAA anti-complement action on LPS-induced DIC in rats were investigated.
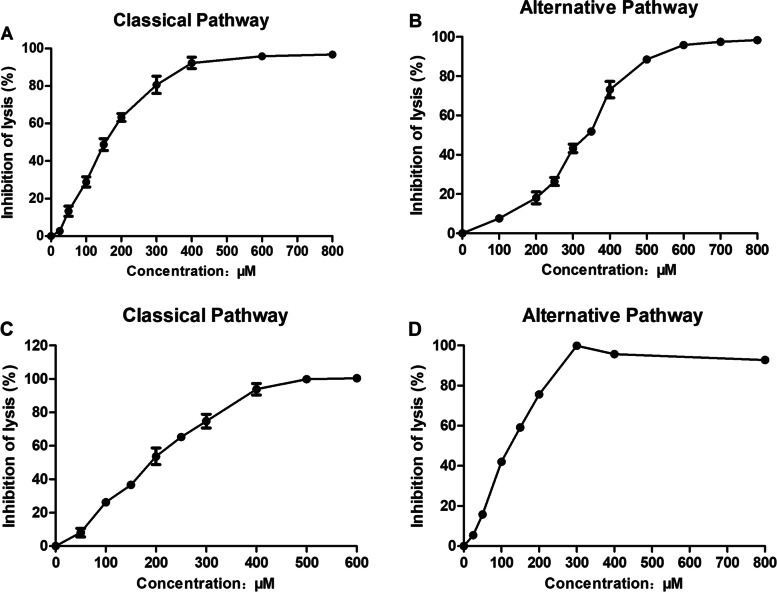
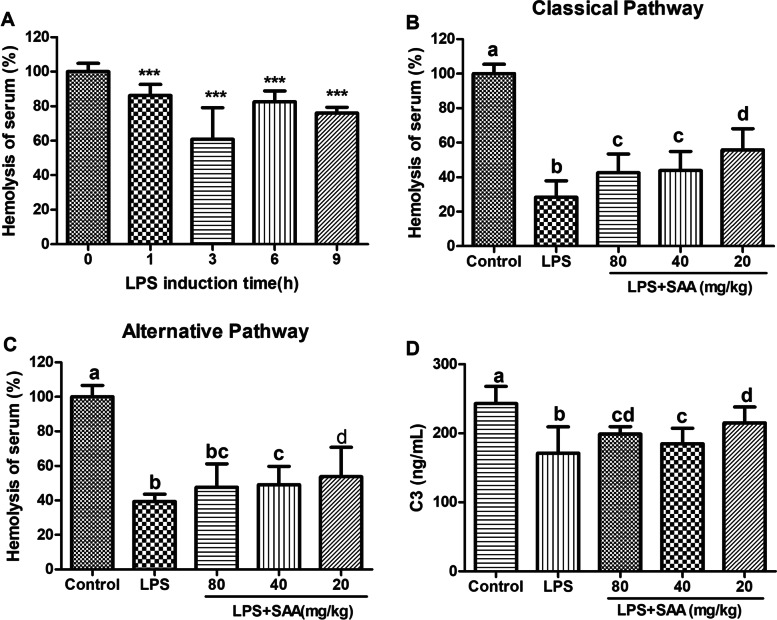
Methods: The complement activity of the classical pathway and alternative pathway was detected through an in vitro hemolysis assay. The binding sites of SAA and complement C3b were predicted by molecular docking. LPS-induced disseminated coagulation experiments were performed on male Wistar rats to assess coagulation function, complement activity, inflammation, biochemistry, blood routine, fibrinolysis, and survival.
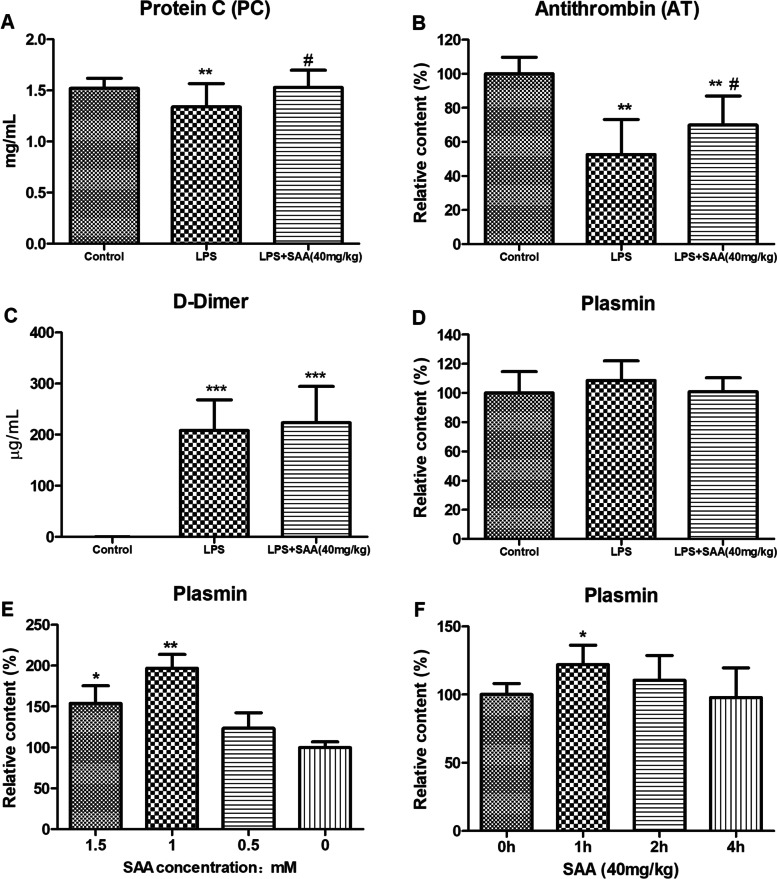
Results: SAA had an anti-complement activity in vivo and in vitro and inhibited the complement activation in the classical and alternative pathway of complement. The infusion of LPS into the rats impaired the coagulation function, increased the plasma inflammatory cytokine level, complemented activation, reduced the clotting factor levels, fibrinogen, and platelets, damaged renal, liver, and lung functions, and led to a high mortality rate (85%). SAA treatment of rats inhibited complement activation and attenuated the significant increase in D-dimer, interleukin-6, alanine aminotransferase, and creatinine. It ameliorated the decrease in plasma levels of fibrinogen and platelets and reversed the decline in activity of protein C and antithrombin III. The treatment reduced kidney, liver, and lung damage, and significantly improved the survival rate of rats (46.2 and 78.6% for the low- and high-dose groups, respectively).
Conclusion: SAA reduced LPS-induced DIC by inhibiting complement activation. It has considerable potential in DIC treatment.
Keywords: C3b; Complement system; Disseminated intravascular coagulation; Lipopolysaccharide; Salvianolic acid A.
© 2022. The Author(s).
Conflict of interest statement
The authors declare that they have no conflicts of interest regarding this work.
Figures





References
MeSH terms
Substances
Grants and funding
LinkOut - more resources
Full Text Sources
