

Pathophysiology of reversible cerebral vasoconstriction syndrome
- PMID: 36127720
- PMCID: PMC9489486
- DOI: 10.1186/s12929-022-00857-4
Pathophysiology of reversible cerebral vasoconstriction syndrome
Abstract
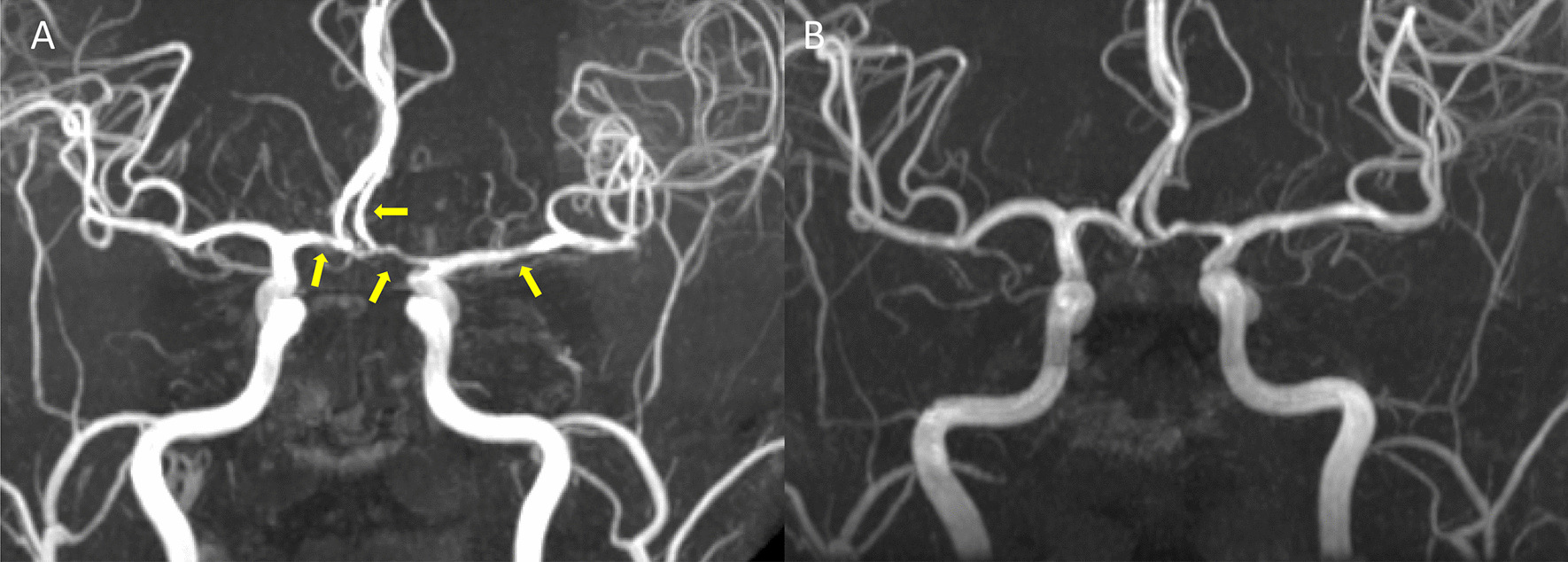
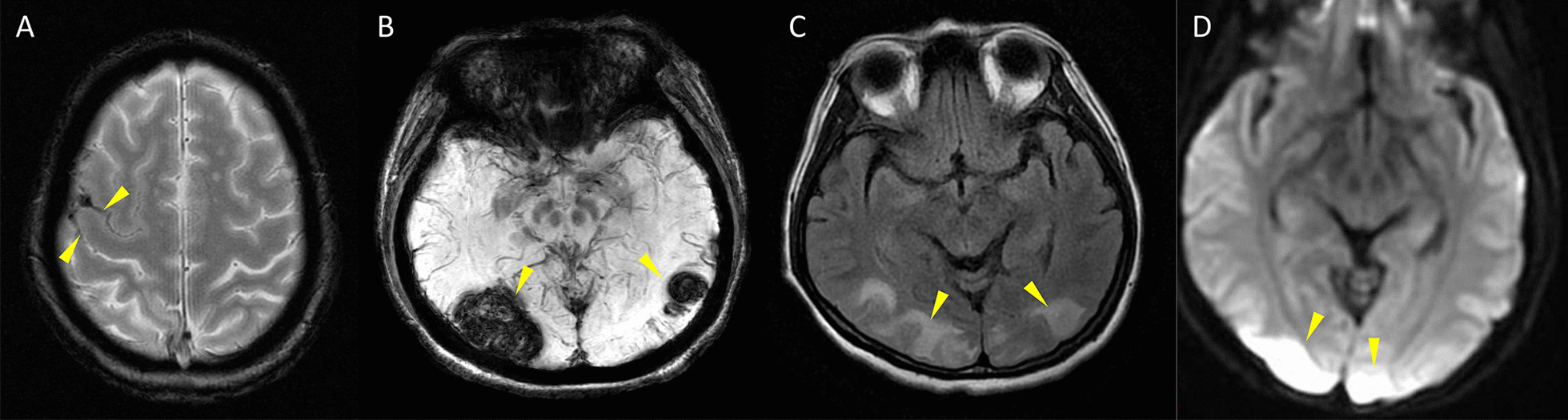
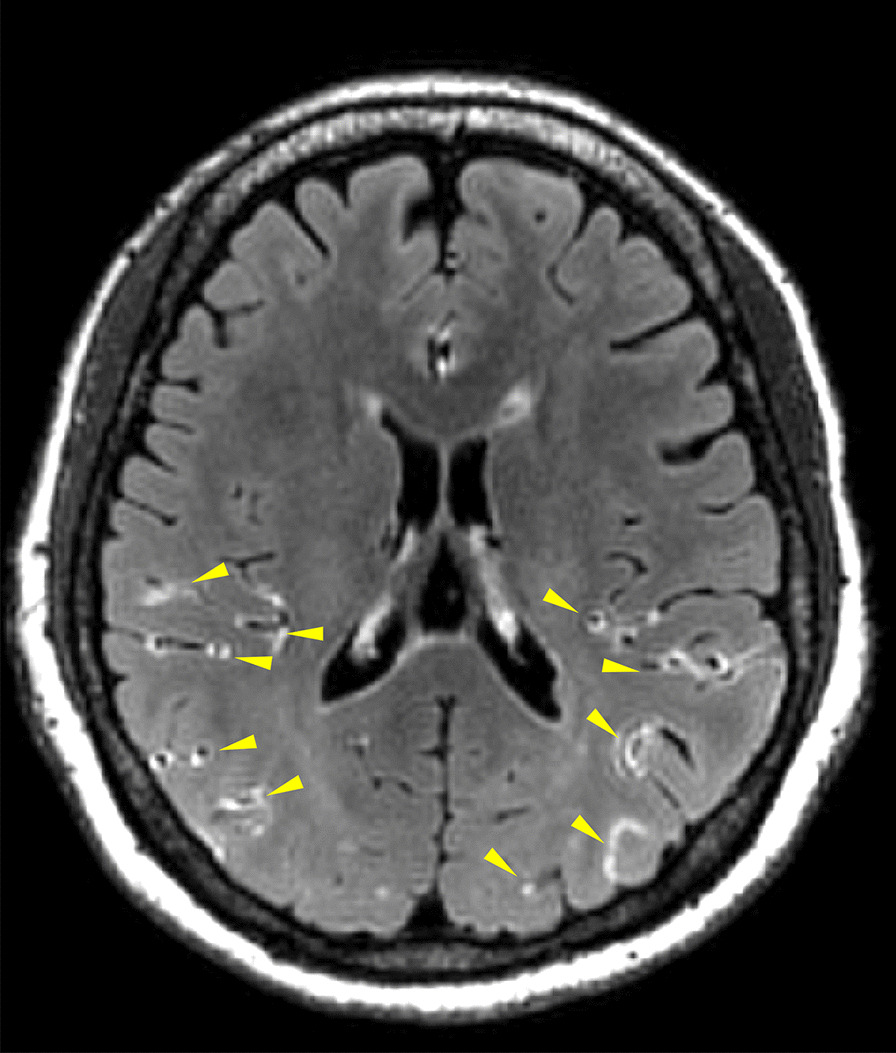
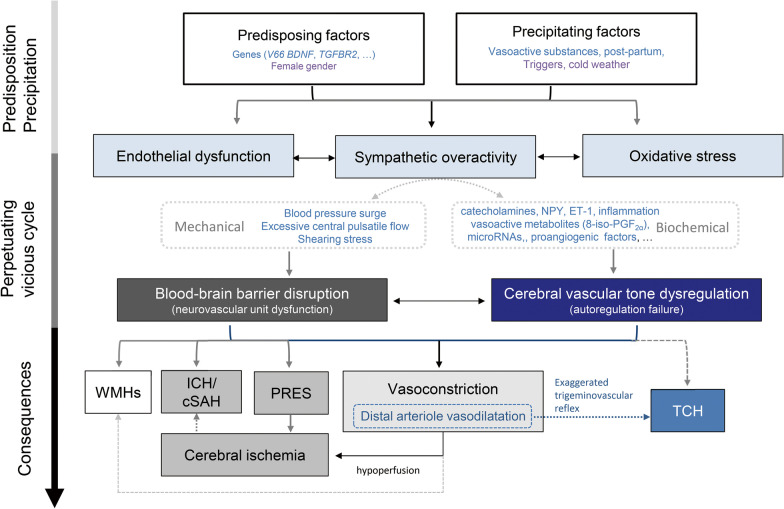
Reversible cerebral vasoconstriction syndrome (RCVS) is a complex neurovascular disorder being recognized during the past two decades. It is characterized by multiple abrupt severe headaches and widespread cerebral vasoconstrictions, with potential complications such as ischemic stroke, convexity subarachnoid hemorrhage, intracerebral hemorrhage and posterior reversible encephalopathy syndrome. The clinical features, imaging findings, and dynamic disease course have been delineated. However, the pathophysiology of RCVS remains elusive. Recent studies have had substantial progress in elucidating its pathogenesis. It is now believed that dysfunction of cerebral vascular tone and impairment of blood-brain barrier may play key roles in the pathophysiology of RCVS, which explains some of the clinical and radiological manifestations of RCVS. Some other potentially important elements include genetic predisposition, sympathetic overactivity, endothelial dysfunction, and oxidative stress, although the detailed molecular mechanisms are yet to be identified. In this review, we will summarize what have been revealed in the literature and elaborate how these factors could contribute to the pathophysiology of RCVS.
Keywords: Blood–brain barrier; Neurovascular unit; Reversible cerebral vasoconstriction syndrome; Thunderclap headache.
© 2022. The Author(s).
Conflict of interest statement
The authors have declared no competing interests.
Figures
References
Publication types
MeSH terms
Grants and funding
- The Featured Areas Research Center Program within the framework of the Higher Education Sprout Project by the Ministry of Education (MOE) in Taiwan/Ministry of Education
- MOST-107-2314-B-010-021/Ministry of Science and Technology (TW)
- 108-2314-B-010-022-MY3/Ministry of Science and Technology (TW)
- 110-2326-B-A49A-501-MY3/Ministry of Science and Technology (TW)
- MOST 108-2321-B-010-014-MY2/Ministry of Science and Technology, Taiwan
- 108-2321-B-010-001-/Ministry of Science and Technology, Taiwan
- 108-2314-B-010-023-MY3/Ministry of Science and Technology, Taiwan
- 110-2321-B-010-005-/Ministry of Science and Technology, Taiwan
- 111-2321-B-A49-004-/Ministry of Science and Technology, Taiwan
- V111C-158/Taipei Veterans General Hospital
- V109D52-001-MY3-3/Taipei Veterans General Hospital
- VGHUST110-G1-3-1/Taipei Veterans General Hospital
- VGH-106-D9-001-MY2-2/Taipei Veterans General Hospital
LinkOut - more resources
Full Text Sources
Miscellaneous
