

Incidence, risk factors, and clinical impact of major bleeding in hospitalized patients with COVID-19: a sub-analysis of the CLOT-COVID Study
- PMID: 36127738
- PMCID: PMC9485792
- DOI: 10.1186/s12959-022-00414-x
Incidence, risk factors, and clinical impact of major bleeding in hospitalized patients with COVID-19: a sub-analysis of the CLOT-COVID Study
Abstract
Background: The coronavirus disease 2019 (COVID-19) causes extensive coagulopathy and a potential benefit of anticoagulation therapy has been documented for prevention of thromboembolic events. Bleeding events has also been reported as a notable complication; whereas, the incidence, risks, and clinical impact of bleeding remain unclear.
Method: The CLOT-COVID Study was a nationwide, retrospective, multicenter cohort study on consecutive hospitalized patients with COVID-19 in Japan between April 2021 and September 2021. In this sub-analysis, we compared the characteristics of patients with and without major bleeding; moreover, we examined the risk factors for and clinical impact of bleeding events.
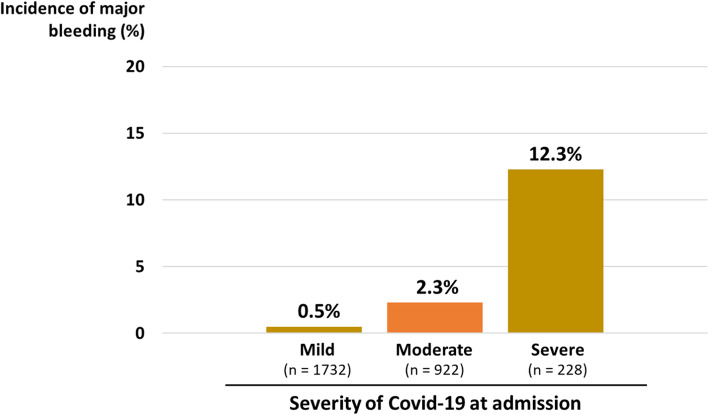
Results: Among 2882 patients with COVID-19, 57 (2.0%) had major bleeding. The incidence of major bleeding increased with COVID-19 severity as follows: 0.5%, 2.3%, and 12.3% in patients with mild, moderate, and severe COVID-19, respectively. COVID-19 severity, history of major bleeding, and anticoagulant type/dose were independently and additively associated with the bleeding incidence. Compared with patients without major bleeding, those with major bleeding exhibited a longer duration of hospitalization (9 [6-14] vs 28 [19-43] days, P < 0.001) and higher mortality during hospitalization (4.9% vs. 35.1%, P < 0.001).
Conclusions: In the real-world clinical practice, the incidence of major bleeding was not uncommon, especially in patients with severe COVID-19. Independent risk factors for major bleeding included history of major bleeding, COVID-19 severity, and anticoagulant use, which could be associated with poor clinical outcomes including higher mortality. Precise recognition of the risks for bleeding may be helpful for an optimal use of anticoagulants and for better outcomes in patients with COVID-19.
Keywords: Anticoagulant; Bleeding; COVID-19; Hospitalization; Mortality; Severity.
© 2022. The Author(s).
Conflict of interest statement
The authors declare that they have no competing interests.
Figures


References
-
- Bikdeli B, Madhavan MV, Jimenez D, Chuich T, Dreyfus I, Driggin E, et al. COVID-19 and thrombotic or thromboembolic disease: Implications for prevention, antithrombotic therapy, and follow-up: JACC State-of-the-Art Review. J Am Coll Cardiol. 2020;75:2950–2973. doi: 10.1016/j.jacc.2020.04.031. - DOI - PMC - PubMed
LinkOut - more resources
Full Text Sources
Miscellaneous
