

Safe surgery for glioblastoma: Recent advances and modern challenges
- PMID: 36127890
- PMCID: PMC9476986
- DOI: 10.1093/nop/npac019
Safe surgery for glioblastoma: Recent advances and modern challenges
Abstract
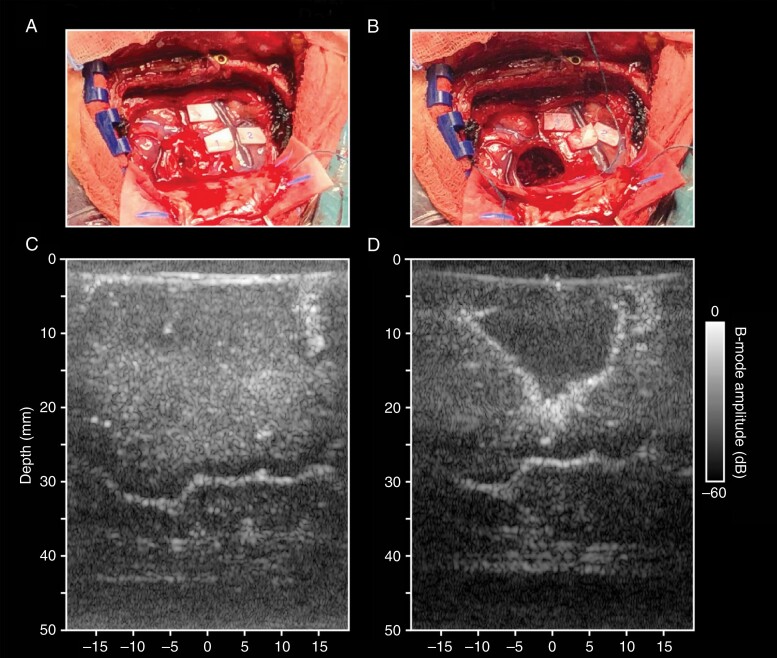
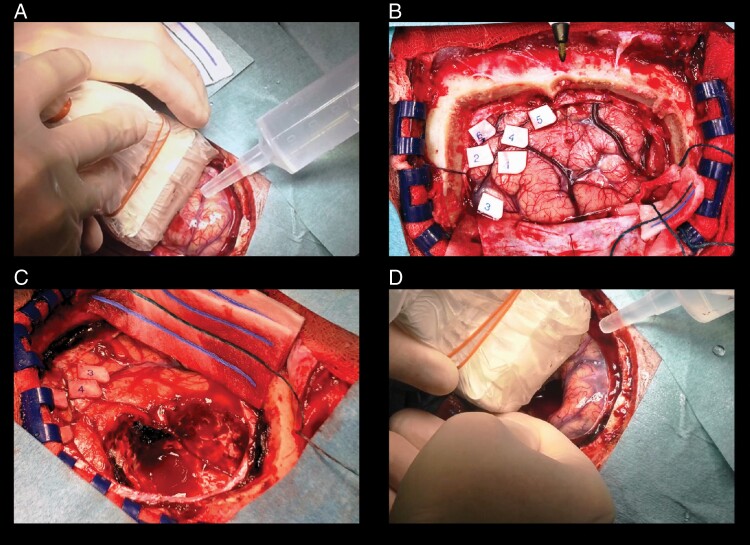
One of the major challenges during glioblastoma surgery is balancing between maximizing extent of resection and preventing neurological deficits. Several surgical techniques and adjuncts have been developed to help identify eloquent areas both preoperatively (fMRI, nTMS, MEG, DTI) and intraoperatively (imaging (ultrasound, iMRI), electrostimulation (mapping), cerebral perfusion measurements (fUS)), and visualization (5-ALA, fluoresceine)). In this review, we give an update of the state-of-the-art management of both primary and recurrent glioblastomas. We will review the latest surgical advances, challenges, and approaches that define the onco-neurosurgical practice in a contemporary setting and give an overview of the current prospective scientific efforts.
Keywords: glioblastoma; imaging; intraoperative mapping; preoperative mapping; review.
© The Author(s) 2022. Published by Oxford University Press on behalf of the Society for Neuro-Oncology and the European Association of Neuro-Oncology.
Figures
References
-
- Ho VK, Reijneveld JC, Enting RH, et al. . Changing incidence and improved survival of gliomas. Eur J Cancer. 2014;50(13):2309–2318. - PubMed
-
- Stupp R, Mason WP, van den Bent MJ, et al. . Radiotherapy plus concomitant and adjuvant temozolomide for glioblastoma. N Engl J Med. 2005;352(10):987–996. - PubMed
-
- Perry JR, Laperriere N, O’Callaghan CJ. Short-course radiation plus temozolomide in elderly patients with glioblastoma. N Engl J Med. 2017;376(11):1027–1037. - PubMed
-
- Stummer W, Meinel T, Pichlmeier U, et al. . Extent of resection and survival in glioblastoma multiforme: identification of and adjustment for bias. Neurosurgery 2008;62(3):564–576. - PubMed
