

Recurrent liponeurocytoma: A case report and systematic review of the literature
- PMID: 36128091
- PMCID: PMC9479547
- DOI: 10.25259/SNI_513_2022
Recurrent liponeurocytoma: A case report and systematic review of the literature
Abstract
Background: Liponeurocytomas are rare neurocytic neoplasms that most often arise in the posterior fossa and affect individuals in the third and fifth decades of life. Most reported cases of this unique tumor in the literature have described a favorable clinical prognosis without recurrence. However, increasing reports of recurrent cases prompted the World Health Organization, in 2016, to recategorize the tumor from Grade I to the less favorable Grade II classification. We conducted a systematic review to identify recurrent cases of this unique tumor and to summarize differences between the primary and recurrent cases of liponeurocytoma.
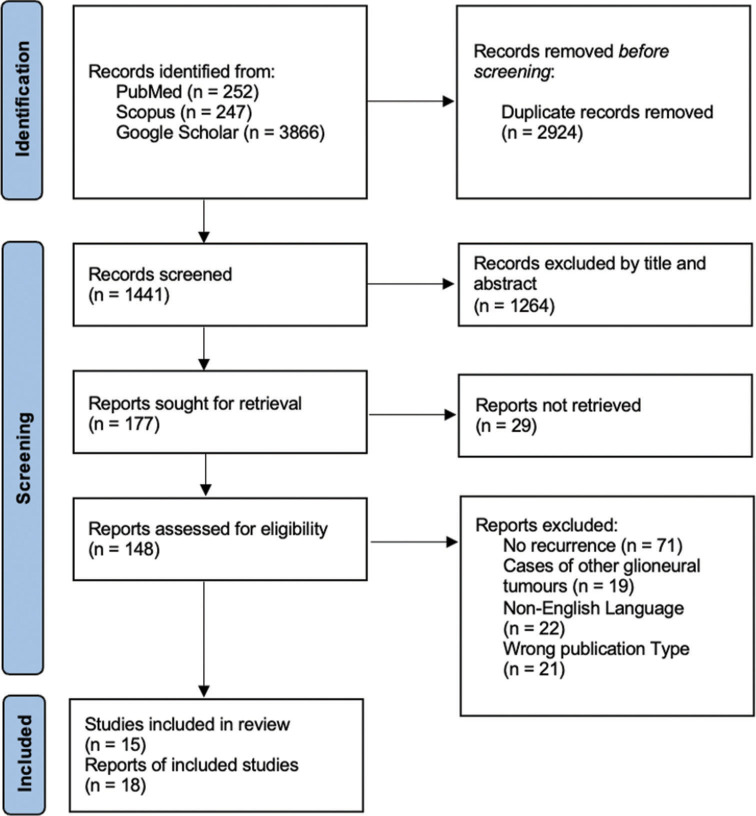
Methods: A systematic review exploring recurrent liponeurocytoma cases was conducted by searching the PubMed, Google Scholar, and Scopus databases for articles in English. Abstracts from articles were read and selected for full-text review according to a priori criteria. Relevant full-text articles were analyzed for symptoms, imaging, location, histological, pathological, treatment, and recurrence-free time between the primary and recurrent cases.
Results: Of 4392 articles, 15 articles accounting for 18 patients were included (level of evidence: IV) in the study. Recurrence-free time decreased from an average of 82 months between the primary tumor resection to first recurrence to 31.3 months between the first and second recurrence. Recurrent tumors demonstrated increased pleomorphic neural cells, necrosis, vascular proliferation, and MIB-1 index when compared to the primary tumor. Several cases also demonstrated decreased lipidizing components when compared to the primary tumor, further indicating increased dedifferentiation. The primary treatment for this tumor was surgical resection with occasional adjunctive radiotherapy.
Conclusion: Recurrent cases of liponeurocytoma have features of increased malignant proliferation compared to the primary cases. The standard treatment for these primary and recurrent tumors is gross total resection. The role of adjunctive radiotherapy remains a matter of debate.
Keywords: Liponeurocytoma; Neurocytic neoplasm; Recurrent; Systematic review.
Copyright: © 2022 Surgical Neurology International.
Conflict of interest statement
There are no conflicts of interest.
Figures
References
-
- Alkadhi H, Keller M, Brandner S, Yonekawa Y, Kollias SS. Neuroimaging of cerebellar liponeurocytoma: Case report. J Neurosurg. 2001;95:324–31. - PubMed
-
- Anghileri E, Eoli M, Paterra R, Ferroli P, Pollo B, Cuccarini V, et al. FABP4 is a candidate marker of cerebellar liponeurocytomas. J Neurooncol. 2012;108:513–9. - PubMed
-
- Bechtel JT, Patton JM, Takei Y. Mixed mesenchymal and neuroectodermal tumor of the cerebellum. Acta Neuropathol. 1978;41:261–3. - PubMed
-
- Bonneville F, Cattin F, Marsot-Dupuch K, Dormont D, Bonneville JF, Chiras J. T1 signal hyperintensity in the sellar region: Spectrum of findings. Radiographics. 2006;26:93–113. - PubMed
Publication types
LinkOut - more resources
Full Text Sources