

Transarterial embolization for convexity dural arteriovenous fistula with or without pial arterial supply: A report of four patients
- PMID: 36128114
- PMCID: PMC9479601
- DOI: 10.25259/SNI_215_2022
Transarterial embolization for convexity dural arteriovenous fistula with or without pial arterial supply: A report of four patients
Abstract
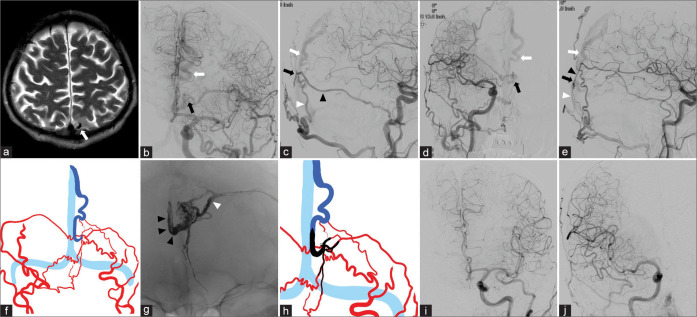
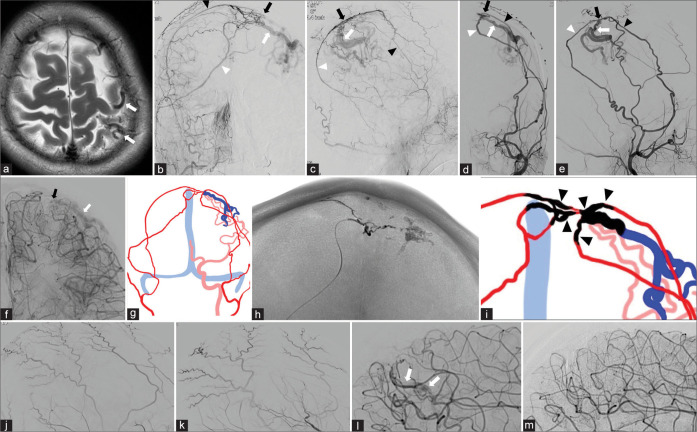
Background: Convexity dural arteriovenous fistulae (dAVF) usually reflux into cortical veins without involving the venous sinuses. Although direct drainage ligation is curative, transarterial embolization (TAE) may be an alternative treatment.
Case description: Between September 2018 and January 2021, we encountered four patients with convexity dAVFs. They were three males and one female; their age ranged from 36 to 73 years. The initial symptom was headache (n = 1) or seizure (n = 2); one patient was asymptomatic. In all patients, the feeders were external carotid arteries with drainage into the cortical veins; in two patients, there was pial arterial supply from the middle cerebral artery. All patients were successfully treated by TAE alone using either Onyx or N-butyl cyanoacrylate embolization. Two patients required two sessions. All dAVFs were completely occluded and follow-up MRI or angiograms confirmed no recurrence.
Conclusion: Our small series suggests that TAE with a liquid embolic material is an appropriate first-line treatment in patients with convexity dAVFs with or without pial arterial supply.
Keywords: Convexity; Dural arteriovenous fistula; Pial artery; Transarterial embolization.
Copyright: © 2022 Surgical Neurology International.
Conflict of interest statement
There are no conflicts of interest.
Figures
Similar articles
-
Microsurgical Findings of Pial Arterial Feeders in Intracranial Dural Arteriovenous Fistulae: A Case Series.Oper Neurosurg. 2020 Nov 16;19(6):691-700. doi: 10.1093/ons/opaa218. Oper Neurosurg. 2020. PMID: 32717026
-
Dural arteriovenous fistulas: a review of the literature and a presentation of a single institution's experience.World Neurosurg. 2013 Jul-Aug;80(1-2):94-102. doi: 10.1016/j.wneu.2012.01.053. Epub 2012 Jan 31. World Neurosurg. 2013. PMID: 22381858
-
Transarterial embolization of clival dural arteriovenous fistulae using liquid embolic agents.Neurosurgery. 2008 Feb;62(2):408-15; discussion 415. doi: 10.1227/01.neu.0000316007.34259.26. Neurosurgery. 2008. PMID: 18382318
-
A Comprehensive Analysis of Dural Arteriovenous Fistula Involving the Superior Sagittal Sinus: A Systematic Review.J Neuroendovasc Ther. 2021;15(1):1-7. doi: 10.5797/jnet.ra.2020-0085. Epub 2020 Sep 8. J Neuroendovasc Ther. 2021. PMID: 37503458 Free PMC article. Review.
-
Medial Tentorial Dural Arteriovenous Fistula Embolization: Single Experience with Embolic Liquid Polymer SQUID and Review of the Literature.World Neurosurg. 2017 Nov;107:1050.e1-1050.e7. doi: 10.1016/j.wneu.2017.08.050. Epub 2017 Aug 18. World Neurosurg. 2017. PMID: 28826865 Review.
Cited by
-
Non-Sinus Type Dural Arteriovenous Fistula: Others.J Neuroendovasc Ther. 2025;19(1):2023-0023. doi: 10.5797/jnet.ra.2023-0023. Epub 2023 Sep 5. J Neuroendovasc Ther. 2025. PMID: 39958458 Free PMC article. Review.
-
Convexity dural arteriovenous fistula with Sylvian-Labbé collateral pattern: A case report.J Cerebrovasc Endovasc Neurosurg. 2024 Dec;26(4):405-411. doi: 10.7461/jcen.2024.E2024.05.001. Epub 2024 Aug 5. J Cerebrovasc Endovasc Neurosurg. 2024. PMID: 39091262 Free PMC article.
References
-
- Borden JA, Wu JK, Shucart WA. A proposed classification for spinal and cranial dural arteriovenous fistulous malformation and implications of treatment. J Neurosurg. 1995;82:166–79. - PubMed
-
- Brinjikji W, Cloft HJ, Lanzino G. Clinical, angiographic, and treatment characteristics of cranial dural arteriovenous fistulas with pial arterial supply. J Neurointerv Surg. 2021;13:331–5. - PubMed
-
- Kato N, Tanaka T, Suzuki Y, Sakamoto H, Arai T, Hasegawa Y, et al. Multistage indocyanine green videoangiography for the convexity dural arteriovenous fistula with angiographically occult pial fistula. J Stroke Cerebrovasc Dis. 2012;21:918.e1–e5. - PubMed
-
- Kobayashi E, Wakamatsu S, Tominaga S. A case of dural arteriovenous malformation on the convexity adjacent to the superior sagittal sinus. No Shinkei Geka. 1994;22:643–8. - PubMed
Publication types
LinkOut - more resources
Full Text Sources