

Contemporary outcome of subsequent pregnancies in patients with previous peripartum cardiomyopathy
- PMID: 36128657
- PMCID: PMC9773727
- DOI: 10.1002/ehf2.14141
Contemporary outcome of subsequent pregnancies in patients with previous peripartum cardiomyopathy
Abstract
Aims: To describe the effect of subsequent pregnancies (SSP) on left ventricular (LV) function and outcomes in patients with peripartum cardiomyopathy (PPCM).
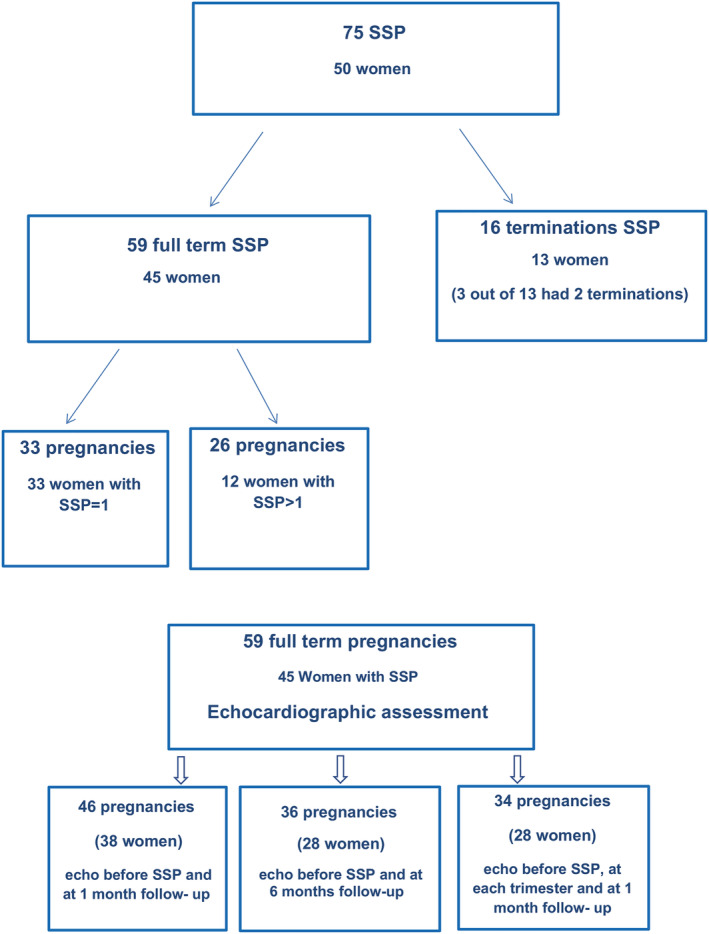
Methods: Among146 women with PPCM who were prospectively followed at two medical centres in Israel (2007-2019), 75 SSPs (in 50 women) were identified: 8 miscarriages, 8 terminations, and 59 life birth.
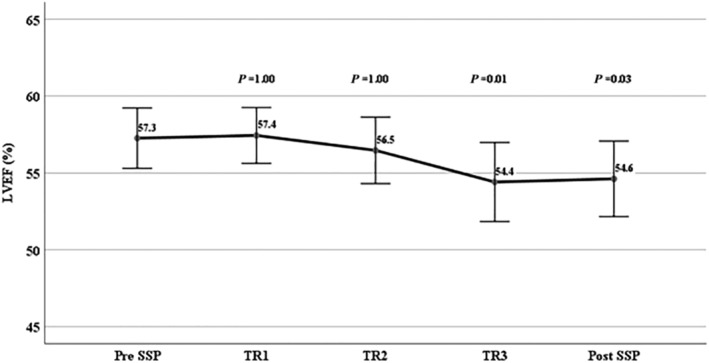
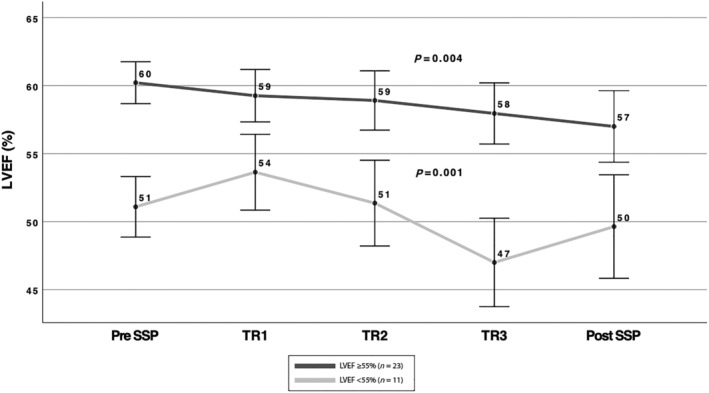
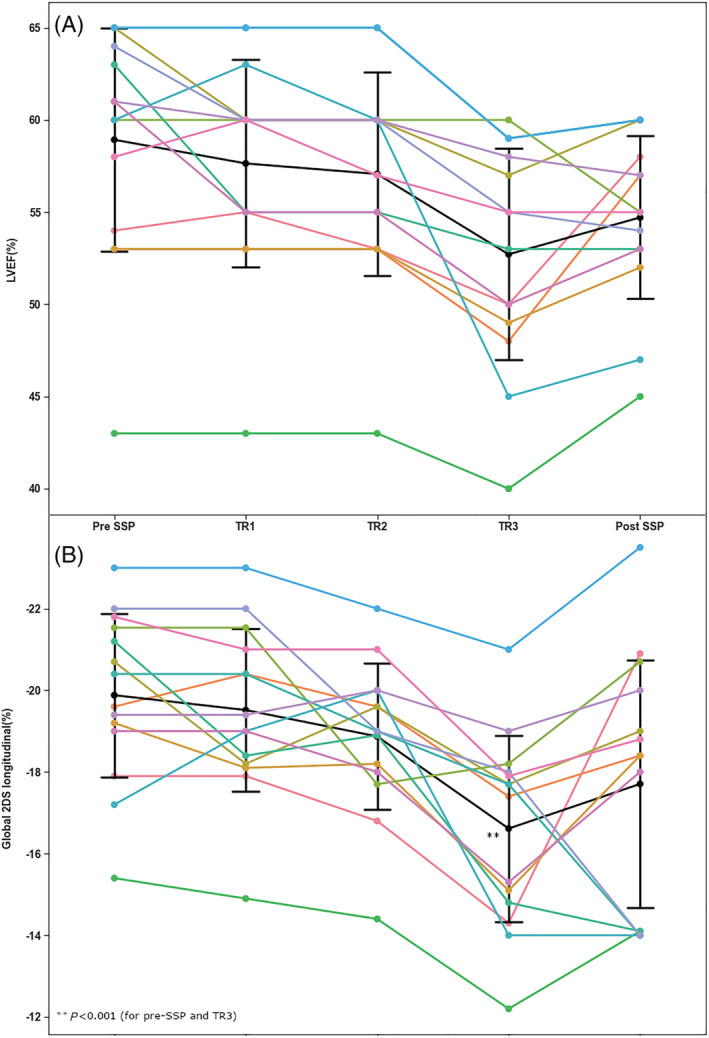
Results: Forty-five patients with 59 full-term SSPs [mean age was 32.9 ± 4.1 years, LV ejection fraction (LVEF) 57.7 ± 5.1%] were analysed. Data on LVEF at 1-month post-delivery were available in 46 and at 6 months in 36 SSPs. There was a small decrease in the mean LVEF, mostly at third trimester (57.2 ± 5.6 vs. 54.4. ± 7.3, P < 0.001); and at 1-mont (57.9 ± 5.7% vs. 55.4 ± 6.1%, P = 0.001) and at 6-month post-delivery (57.4 ± 6.1 vs. 55.3 ± 7.9%, P = 0.03). In patients with pre-SSP LV LVEF ≥55%, a mild reduction in the mean group LVEF was seen at 1-month post-delivery (P = 0.009). One patient with pre-SSP LVEF ≥55% developed severe relapse. In patients with pre-SSP LVEF <55%, a mild reduction in LVEF was obtained mostly at third trimester (51.1 ± 5.6 vs 47.0 ± 7.4%, P < 0.001), which persisted at 6 months (P = 0.03). A relapse was observed in three (25%) women with LVEF <55%. There was no maternal mortality, 32 patients delivered by caesarean section, and there were no foetal complications.
Conclusions: Our study indicates a favourable outcome and low likelihood of maternal mortality associated with SSP in women with a history of PPCM and recovered LV systolic function. SSP was associated with a slight reduction in LVEF mostly during the third trimester, which persisted up to 6 months after delivery.
Keywords: Cardiomyopathy; Outcome; Peripartum; Pregnancies; Subsequent.
© 2022 The Authors. ESC Heart Failure published by John Wiley & Sons Ltd on behalf of European Society of Cardiology.
Conflict of interest statement
None declared.
Figures
References
-
- Sliwa K, Petrie MC, Hilfiker‐Kleiner D, Mebazaa A, Jackson A, Johnson MR, van der Meer P, Mbakwem A, Bauersachs J. Long‐term prognosis, subsequent pregnancy, contraception and overall management of peripartum cardiomyopathy: Practical guidance paper from the Heart Failure Association of the European Society of Cardiology Study Group on peripartum cardiomyopathy. Eur J Heart Fail. 2018; 20: 951–962. - PubMed
-
- Fett JD, Fristoe KL, Welsh SN. Risk of heart failure relapse in subsequent pregnancy among peripartum cardiomyopathy mothers. Int J Gynaecol Obstet. 2010; 109: 34–36. - PubMed
-
- Elkayam U, Tummala PP, Rao K, Akhter MW, Karaalp IS, Wani OR, Hameed A, Gviazda I, Shotan A. Maternal and fetal outcomes of subsequent pregnancies in women with peripartum cardiomyopathy. N Engl J Med. 2001; 344: 1567–1571. - PubMed
-
- Elkayam U. Risk of subsequent pregnancy in women with a history of peripartum cardiomyopathy. J Am Coll Cardiol. 2014; 64: 1629–1636. - PubMed
MeSH terms
LinkOut - more resources
Full Text Sources
Medical