

Genomic profiling for clinical decision making in myeloid neoplasms and acute leukemia
- PMID: 36130297
- PMCID: PMC10488320
- DOI: 10.1182/blood.2022015853
Genomic profiling for clinical decision making in myeloid neoplasms and acute leukemia
Abstract
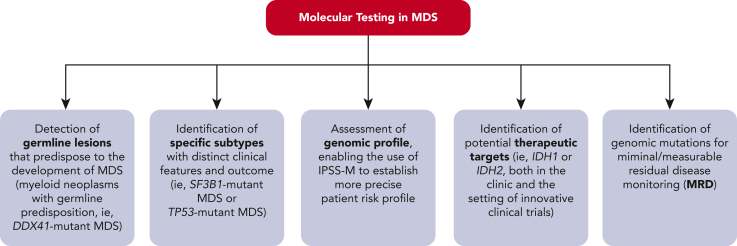
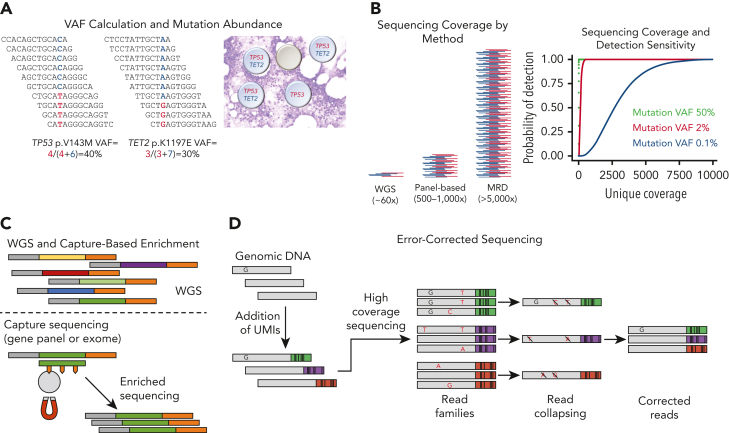
Myeloid neoplasms and acute leukemias derive from the clonal expansion of hematopoietic cells driven by somatic gene mutations. Although assessment of morphology plays a crucial role in the diagnostic evaluation of patients with these malignancies, genomic characterization has become increasingly important for accurate diagnosis, risk assessment, and therapeutic decision making. Conventional cytogenetics, a comprehensive and unbiased method for assessing chromosomal abnormalities, has been the mainstay of genomic testing over the past several decades and remains relevant today. However, more recent advances in sequencing technology have increased our ability to detect somatic mutations through the use of targeted gene panels, whole-exome sequencing, whole-genome sequencing, and whole-transcriptome sequencing or RNA sequencing. In patients with myeloid neoplasms, whole-genome sequencing represents a potential replacement for both conventional cytogenetic and sequencing approaches, providing rapid and accurate comprehensive genomic profiling. DNA sequencing methods are used not only for detecting somatically acquired gene mutations but also for identifying germline gene mutations associated with inherited predisposition to hematologic neoplasms. The 2022 International Consensus Classification of myeloid neoplasms and acute leukemias makes extensive use of genomic data. The aim of this report is to help physicians and laboratorians implement genomic testing for diagnosis, risk stratification, and clinical decision making and illustrates the potential of genomic profiling for enabling personalized medicine in patients with hematologic neoplasms.
© 2022 by The American Society of Hematology.
Conflict of interest statement
Conflict-of-interest disclosure: E.J.D. is a consultant for Cofactor Genomics, Genescopy LLC, and Vertex, and has received honoraria from Blueprint bio and AbbVie. C.D. research support (to institution): AbbVie, Astex, BMS, Beigene, Cleave, Foghorn, ImmuneOnc, Loxo, Servier Consultant with honoraria: Abbvie, BMS, Foghorn, GSK, Jazz, Novartis, Notable Labs, Servier, Takeda. I.I. received honoraria from Amgen and Mission Bio. S.J. received consulting fees from Novartis, Roche Genentech, AVRO Bio, and Foresite Labs; speaking fees from GSK; is an equity holder and on the scientific advisory board of Bitterroot Bio; and is a founder, equity holder, and scientific advisory board member of TenSixteen Bio. A.M.V. received an advisory board and lecture fee from Novartis, AbbVie, Incyte, Blueprint, BMS, and GSK. K.P.P. has served as consultant for Novartis and Astellas and received speaker fees from Astella. M.E.A. received honoraria from Janssen Global Services, Bristol-Myers Squibb, AstraZeneca, Roche, Biocartis, Invivoscribe, Physician Educational Resources, Peerview Institute for Medical Education, Clinical Care Options, and RMEI Medical Education. R.B. is employed by and owns stocks in Aptose Biosciences; ad-hoc advisory board for BMS; DMC chair for Gilead and Epizyme; and received research funding from Takeda. M.B. serves on advisory boards for Amgen and Blueprint Medicines. S.B. is a member of the advisory board of Qiagen, Novartis, and Cepheid; received honoraria from Qiagen, Novartis, Bristol-Myers Squibb, and Cepheid; and received research support from Novartis and Cepheid. C.A.C. serves on the advisory board for Novartis and AOP Orphan and received research funding from BMS. H.D. consults with honoraria for AbbVie, Agios, Amgen, Astellas, AstraZeneca, Berlin-Chemie, BMS, Celgene, GEMoaB, Gilead, Janssen, Jazz, Novartis, Servier, and Syndax and received clinical research funding (to institution) from AbbVie, Agios, Amgen, Astellas, Bristol Myers Squibb, Celgene, Jazz Pharmaceuticals, Kronos Bio, and Novartis. R.K. is a speaker bureau and advisory board member of AbbVie; received a research grant from and serves on advisory board of BMS; is a speaker bureau and advisory board member of CTI biopharma; consults for Geron; is a speaker bureau and advisory board member of Jazz; is an advisory board member of Novartis and Taiho; and is a speaker bureau and advisory board member of PharmaEssentia and Servio. S.L. has received advisory fees from AbbVie, Blue Print Medicine, Daiichi Sankyo, Guidepoint; is a consultant for Gerson Lehrman Group, Qual World, Guidepoint; has received honoraria from Path Education Partners, Pathology Learning Center, Peer View; has stock ownership in AbbVie; has research support from Astellas, Amgen. C.G.M. received research funding from Loxo Oncology, Pfizer, AbbVie; received honoraria from Amgen and Illumina; and holds stock in Amgen. E.P. is a founder, equity holders and hold fiduciary roles in Isabl Inc as well as has scientific advisor shares in ten sixteen bio. D.M.R. received honoraria from Novartis, BMS, and Keros. B.L.E. has received research funding from Celgene, Deerfield, Novartis, and Calico and consulting fees from GRAIL; and is a member of the scientific advisory board and shareholder for Neomorph Therapeutics, TenSixteen Bio, Skyhawk Therapeutics, and Exo Therapeutics. The remaining authors declare no competing financial interests.
Figures


References
-
- Granada I, Palomo L, Ruiz-Xiville N, Mallo M, Sole F. Cytogenetics in the genomic era. Best Pract Res Clin Haematol. 2020;33(3):607–616. - PubMed
-
- Mallo M, Arenillas L, Espinet B, et al. Fluorescence in situ hybridization improves the detection of 5q31 deletion in myelodysplastic syndromes without cytogenetic evidence of 5q. Haematologica. 2008;93(7):1001–1008. - PubMed
-
- Coleman JF, Theil KS, Tubbs RR, Cook JR. Diagnostic yield of bone marrow and peripheral blood FISH panel testing in clinically suspected myelodysplastic syndromes and/or acute myeloid leukemia: a prospective analysis of 433 cases. Am J Clin Pathol. 2011;135(6):915–920. - PubMed
Publication types
MeSH terms
Grants and funding
LinkOut - more resources
Full Text Sources
Medical
Miscellaneous
