

Extended resection for seizure control of pure motor strip focal cortical dysplasia during awake craniotomy: illustrative case
- PMID: 36130534
- PMCID: PMC9379631
- DOI: 10.3171/CASE21605
Extended resection for seizure control of pure motor strip focal cortical dysplasia during awake craniotomy: illustrative case
Abstract
Background: Focal cortical dysplasias (FCD) represent highly intrinsically epileptogenic lesions that require complete resection for seizure control. Resection of pure motor strip FCD can be challenging. Effective control of postoperative seizures is crucial and extending the boundaries of resection in an eloquent zone remains controversial.
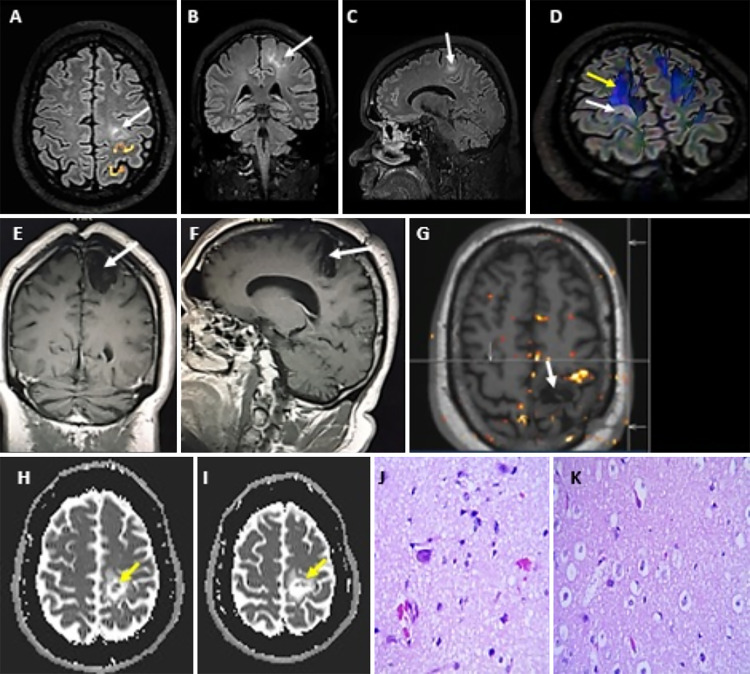
Observations: The authors report a 52-year-old right-handed male with refractory epilepsy. The seizure phenotype was a focal crisis with preserved awareness and a clonic motor onset of right-hemibody. Epilepsy surgery protocol demonstrated a left pure motor strip FCD and a full-awake resective procedure with motor brain mapping was performed. Further resection of surgical boundaries monitoring function along intraoperative motor tasks with no direct electrical stimulation corroborated by intraoperative-neuromonitorization was completed as the final part of the surgery. In the follow-up period of 3-years, the patient has an Engel-IB seizure-control with mild distal lower limb palsy and no gate compromise.
Lessons: This report represents one of the few cases with pure motor strip FCD resection. In a scenario similar to this case, the authors consider that this variation can be useful to improve seizure control and the quality of life of these patients by extending the resection of a more extensive epileptogenic zone minimizing functional damage.
Keywords: awake craniotomy; brain mapping; epilepsy surgery; focal cortical dysplasia.
Conflict of interest statement
Figures
Similar articles
-
Epilepsy surgery for focal cortical dysplasia: Seizure and quality of life (QOLIE-89) outcomes.Neurol India. 2018 Nov-Dec;66(6):1655-1666. doi: 10.4103/0028-3886.246263. Neurol India. 2018. PMID: 30504559
-
Seizure outcome following primary motor cortex-sparing resective surgery for perirolandic focal cortical dysplasia.Int J Surg. 2016 Dec;36(Pt B):466-476. doi: 10.1016/j.ijsu.2015.10.036. Epub 2015 Nov 2. Int J Surg. 2016. PMID: 26542986 Review.
-
The role of intraoperative MRI in resective epilepsy surgery for peri-eloquent cortex cortical dysplasias and heterotopias in pediatric patients.Neurosurg Focus. 2016 Mar;40(3):E16. doi: 10.3171/2016.1.FOCUS15538. Neurosurg Focus. 2016. PMID: 26926056
-
Awake craniotomy for epilepsy surgery on eloquent speech areas: a single-centre experience.Epileptic Disord. 2021 Apr 1;23(2):347-356. doi: 10.1684/epd.2021.1275. Epileptic Disord. 2021. PMID: 33926856
-
Left Frontal Meningioangiomatosis Associated with Type IIIc Focal Cortical Dysplasia Causing Refractory Epilepsy and Literature Review.World Neurosurg. 2018 Jun;114:281-288. doi: 10.1016/j.wneu.2018.03.145. Epub 2018 Mar 30. World Neurosurg. 2018. PMID: 29605698 Review.
Cited by
-
An update on tests used for intraoperative monitoring of cognition during awake craniotomy.Acta Neurochir (Wien). 2024 May 7;166(1):204. doi: 10.1007/s00701-024-06062-6. Acta Neurochir (Wien). 2024. PMID: 38713405 Free PMC article.
-
Intraoperative monitoring during awake craniotomy for glioblastoma resection in the second trimester of pregnancy. A case report and literature review.Clin Neurophysiol Pract. 2025 Feb 28;10:63-69. doi: 10.1016/j.cnp.2025.02.006. eCollection 2025. Clin Neurophysiol Pract. 2025. PMID: 40124178 Free PMC article.
References
-
- Raabe A, Beck J, Schucht P, Seidel K. Continuous dynamic mapping of the corticospinal tract during surgery of motor eloquent brain tumors: evaluation of a new method. J Neurosurg. 2014;120(5):1015–1024. - PubMed
-
- Szelényi A, Bello L, Duffau H, et al. Intraoperative electrical stimulation in awake craniotomy: methodological aspects of current practice. Neurosurg Focus. 2010;28(2):E7. - PubMed
-
- Landazuri P, Eccher M. Simultaneous direct cortical motor evoked potential monitoring and subcortical mapping for motor pathway preservation during brain tumor surgery: is it useful? J Clin Neurophysiol. 2013;30(6):623–625. - PubMed
-
- Shiban E, Krieg SM, Haller B, et al. Intraoperative subcortical motor evoked potential stimulation: how close is the corticospinal tract? J Neurosurg. 2015;123(3):711–720. - PubMed
-
- Seidel K, Beck J, Stieglitz L, Schucht P, Raabe A. The warning-sign hierarchy between quantitative subcortical motor mapping and continuous motor evoked potential monitoring during resection of supratentorial brain tumors. J Neurosurg. 2013;118(2):287–296. - PubMed
LinkOut - more resources
Full Text Sources
