

Tissue Healing in Hemicraniectomy
- PMID: 36133503
- PMCID: PMC9482351
- DOI: 10.7759/cureus.29260
Tissue Healing in Hemicraniectomy
Abstract
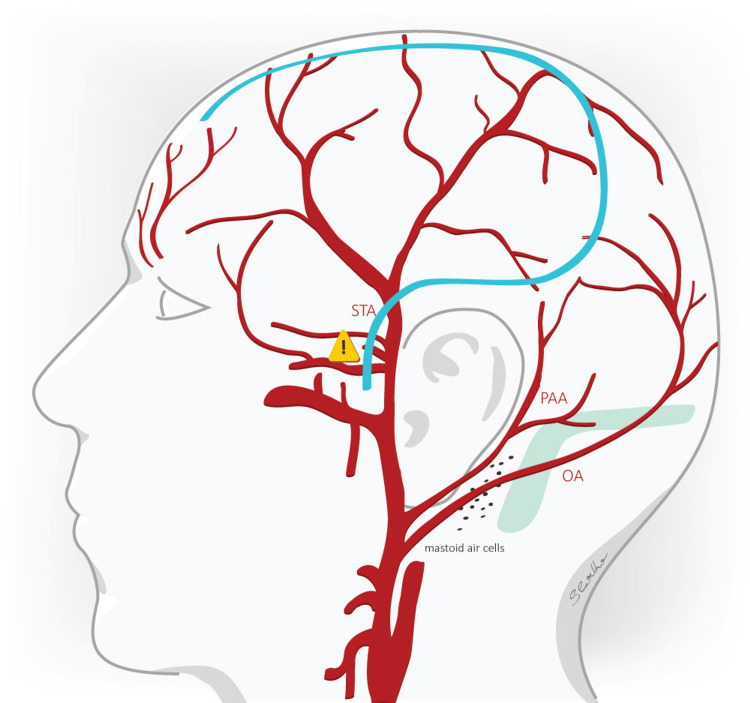
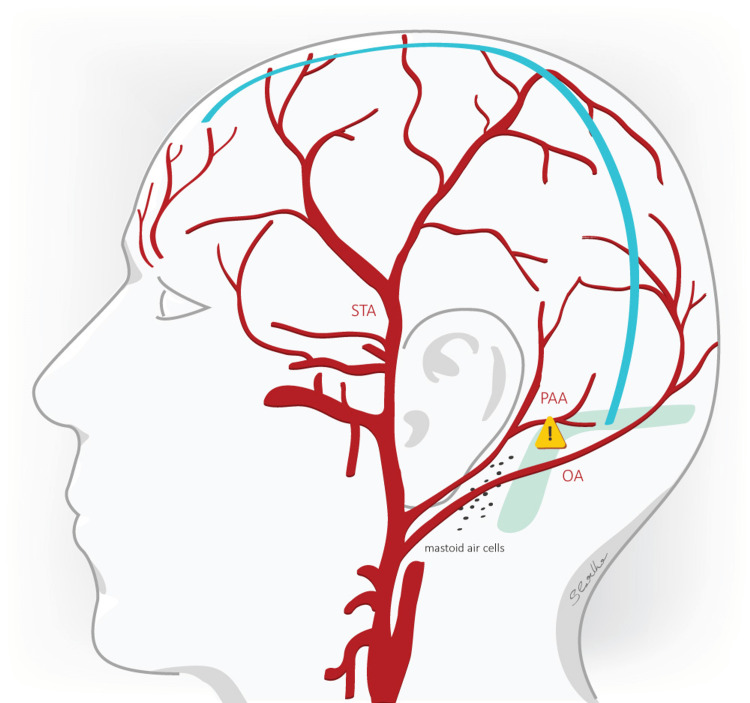
Introduction Decompressive hemicraniectomy (DHC) is a last-resort treatment for refractory intracranial hypertension. Perioperative morbidity is associated with high risks of wound healing disturbances (WHD). Recently, a retromastoidal frontoparietooccipital (RMF) incision type was performed to avoid healing disturbance due to enhanced tissue flap perfusion compared to the classical reverse "question mark" ("Dandy flap") incision. The goal of this study was to analyze the details of tissue healing problems in DHC. Materials and methods A total of 60 patients who underwent DHC were retrospectively analyzed. In 30 patients the "Dandy flap" incision (group A) and in 30 patients the RMF incision (group B) was made. Since no evidence-based data for the incision type that favors better wound healing exists, the form of incision was left at the surgeon´s discretion. Documentation of the patients was screened for the incidence of WHD: wound necrosis, dehiscence, and cerebrospinal fluid (CSF) leakage. Patient age, the time interval from surgery until the appearance of WHD, the length of surgeries in minutes, and the indications of the DHC were analyzed. A Chi-square test of independence was performed to examine the relationship between the incision type and the appearance of WHD with the statistical significance level set at p<0.05. The mean age of the patients, the mean time interval from surgery until the occurrence of WHD, and the mean length of the surgery between the two groups were compared using an independent sample t-test with the statistical significance level set at p<0.05. Results The most common indication for DHC in both groups was malignant MCA infarction (n=20, 66.6% for group A and n=16, 53.3% for group B). CSF leakage was 20% of the most frequent WHD in each group. Wound necrosis was observed only in group A. Although group B showed 13.3% fewer WHD than group A, this difference was not statistically significant. There was no statistically significant difference in the time range between surgery and the occurrence of WHD between the two groups. The length of surgery in group B was significantly shorter than in group A (120.2 mins vs. 103.7 mins). Conclusion A noticeable trend for reduced WHD was observed in the patient group using the RMF incision type although the difference was not statistically significant. We praise that the RMF incision allows an optimized skin-flap vascularization and, thereby, facilitates better wound healing. We were able to show a statistically shorter length of surgery with the RMF incision in contrast to the classic "Dandy flap" incision. Larger multicenter studies should be implemented to analyze and address the major advantages and pitfalls of the routinely applied incision techniques.
Keywords: dandyflap; emergency neurosurgery; hemicraniectomy; retromastoidal (rmf) incision; tissue healing.
Copyright © 2022, Nerntengian et al.
Conflict of interest statement
The authors have declared that no competing interests exist.
Figures
References
-
- Cranioplasty after decompressive hemicraniectomy: underestimated surgery-associated complications? Wachter D, Reineke K, Behm T, Rohde V. Clin Neurol Neurosurg. 2013;115:1293–1297. - PubMed
-
- Invasive monitoring of intracranial pressure after decompressive craniectomy in malignant stroke. Hernández-Durán S, Meinen L, Rohde V, von der Brelie C. Stroke. 2021;52:707–711. - PubMed
-
- Decompressive hemicraniectomy in malignant middle cerebral artery infarction: the 'real world' beyond studies. Pledl HW, Hoyer C, Rausch J, et al. Eur Neurol. 2016;76:48–56. - PubMed
-
- Marked reduction in wound complication rates following decompressive hemicraniectomy with an improved operative closure technique. Sughrue ME, Bloch OG, Manley GT, Stiver SI. J Clin Neurosci. 2011;18:1201–1205. - PubMed
-
- Technical aspects of decompressive craniectomy for malignant middle cerebral artery infarction. Johnson RD, Maartens NF, Teddy PJ. J Clin Neurosci. 2011;18:1023–1027. - PubMed
LinkOut - more resources
Full Text Sources