

Evaluation of a Navigated 3D Ultrasound Integration for Brain Tumor Surgery: First Results of an Ongoing Prospective Study
- PMID: 36135087
- PMCID: PMC9498154
- DOI: 10.3390/curroncol29090518
Evaluation of a Navigated 3D Ultrasound Integration for Brain Tumor Surgery: First Results of an Ongoing Prospective Study
Abstract
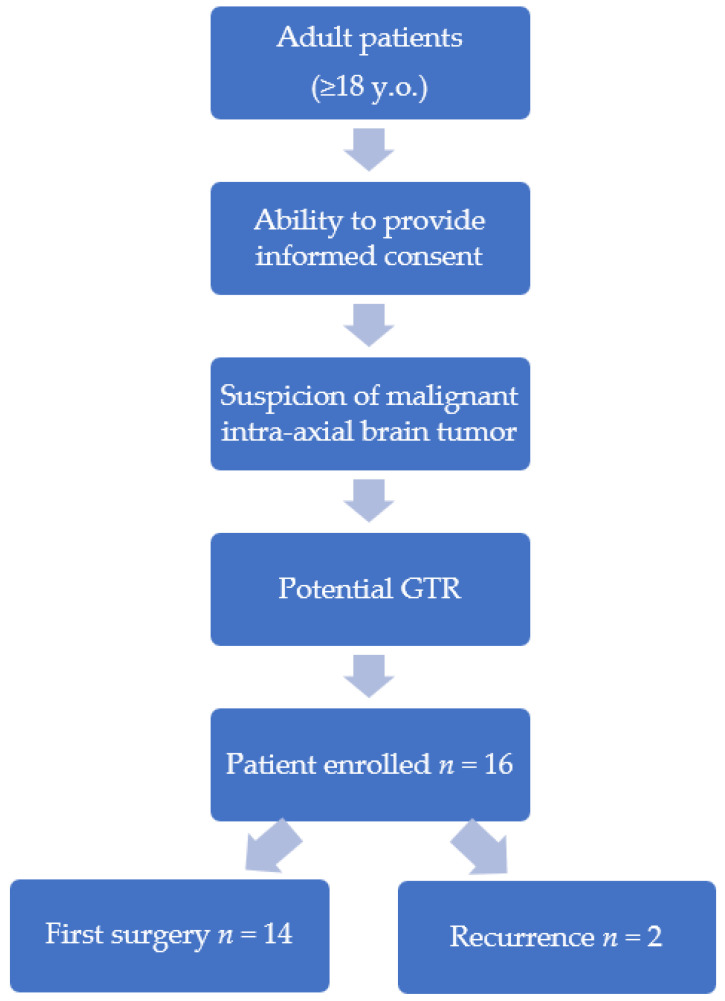
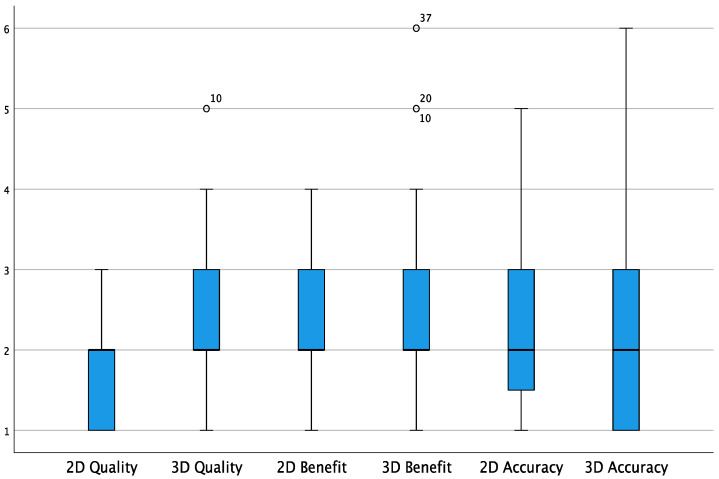
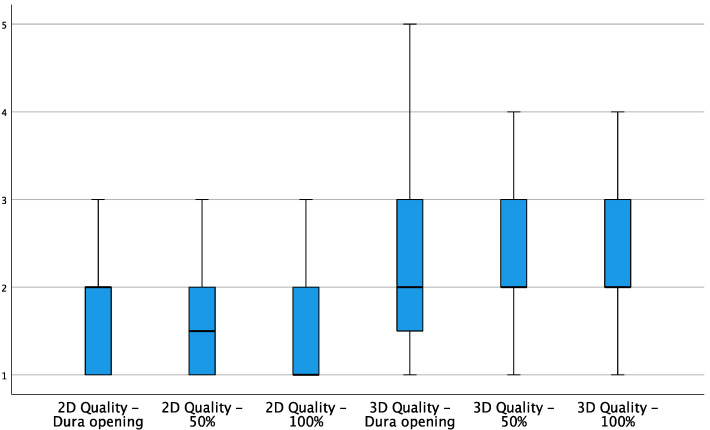
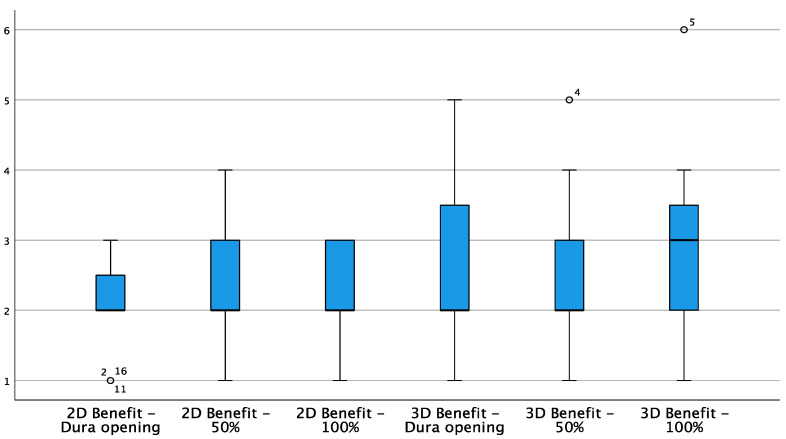
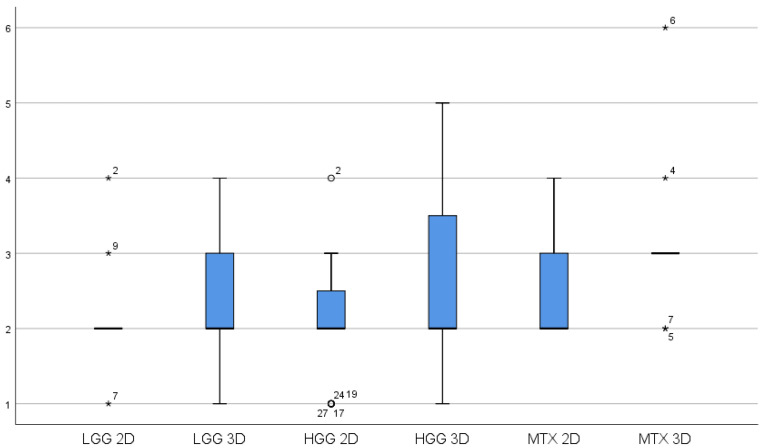
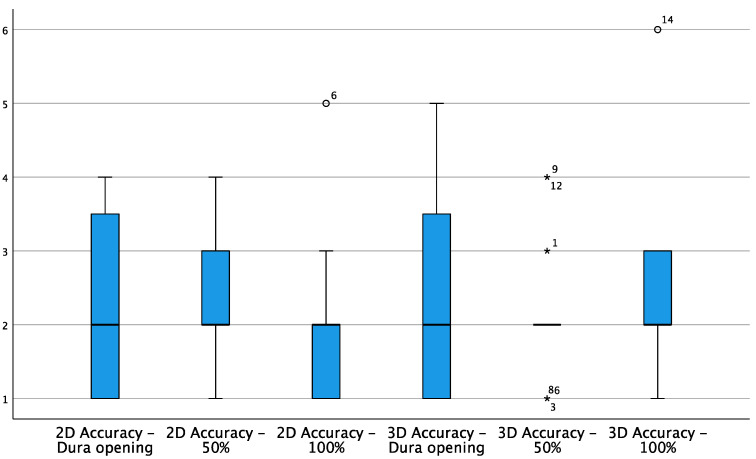
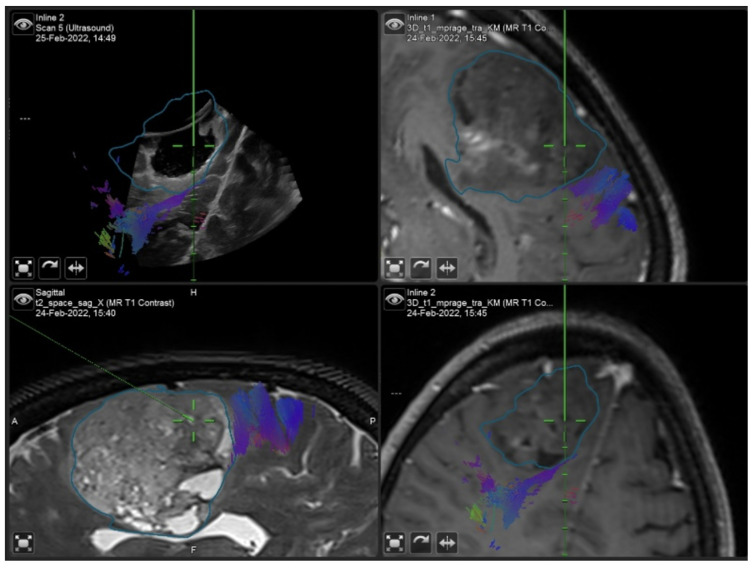
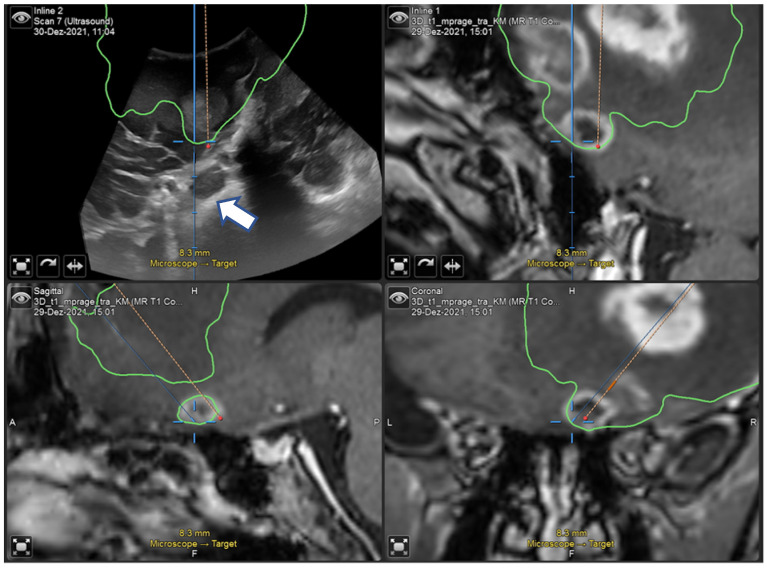
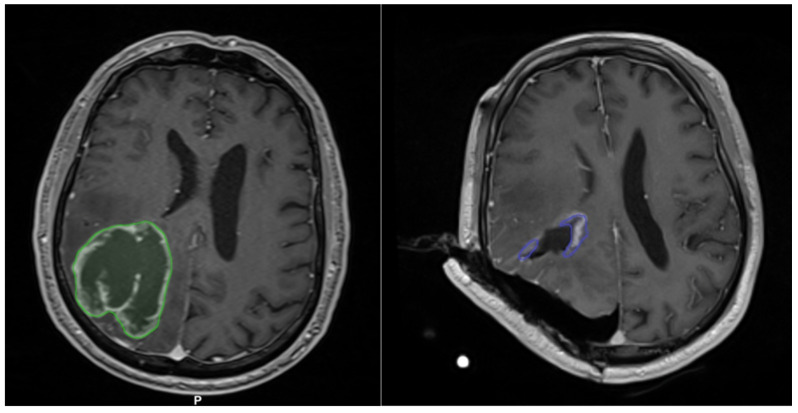
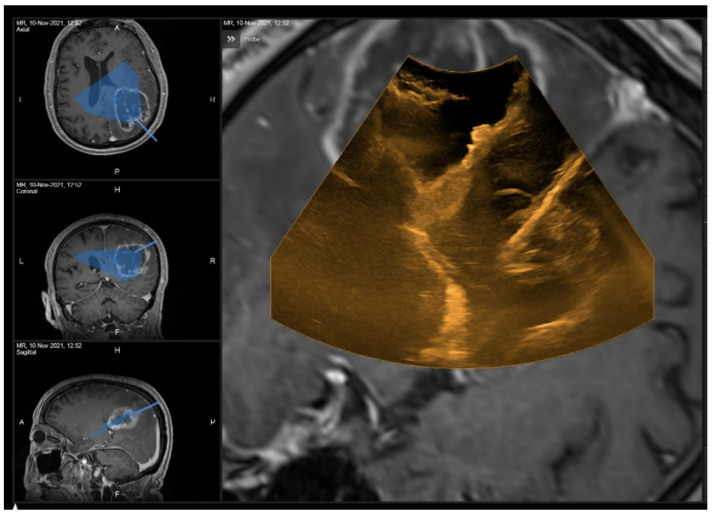
The aim of the study was to assess the quality, accuracy and benefit of navigated 2D and 3D ultrasound for intra-axial tumor surgery in a prospective study. Patients intended for gross total resection were consecutively enrolled. Intraoperatively, a 2D and 3D iUS-based resection was performed. During surgery, the image quality, clinical benefit and navigation accuracy were recorded based on a standardized protocol using Likert’s scales. A total of 16 consecutive patients were included. Mean ratings of image quality in 2D iUS were significantly higher than in 3D iUS (p < 0.001). There was no relevant decrease in rating during the surgery in 2D and 3D iUS (p > 0.46). The benefit was rated 2.2 in 2D iUS and 2.6 in 3D iUS (p = 0.08). The benefit remained stable in 2D, while there was a slight decrease in the benefit in 3D after complete tumor resection (p = 0.09). The accuracy was similar in both (mean 2.2 p = 0.88). Seven patients had a small tumor remnant in intraoperative MRT (mean 0.98 cm3) that was not appreciated with iUS. Crucially, 3D iUS allows for an accurate intraoperative update of imaging with slightly lower image quality than 2D iUS. Our preliminary data suggest that the benefit and accuracy of 2D and 3D iUS navigation do not undergo significant variations during tumor resection.
Keywords: extent of resection; glioma surgery; image quality; intraoperative 3D ultrasound; navigation.
Conflict of interest statement
A.P. (Andrej Pala) and J.C. are working as Brainlab consultants.
Figures
Similar articles
-
Navigated 3-Dimensional Intraoperative Ultrasound for Spine Surgery.World Neurosurg. 2019 Nov;131:e155-e169. doi: 10.1016/j.wneu.2019.07.188. Epub 2019 Jul 31. World Neurosurg. 2019. PMID: 31376550
-
3D intra-operative ultrasound and MR image guidance: pursuing an ultrasound-based management of brainshift to enhance neuronavigation.Int J Comput Assist Radiol Surg. 2017 Oct;12(10):1711-1725. doi: 10.1007/s11548-017-1578-5. Epub 2017 Apr 8. Int J Comput Assist Radiol Surg. 2017. PMID: 28391583
-
Navigated Intraoperative Ultrasound Offers Effective and Efficient Real-Time Analysis of Intracranial Tumor Resection and Brain Shift.Oper Neurosurg. 2025 Feb 1;28(2):148-158. doi: 10.1227/ons.0000000000001250. Epub 2024 Jul 12. Oper Neurosurg. 2025. PMID: 38995025
-
3D ultrasound-guided resection of low-grade gliomas: principles and clinical examples.Neurosurg Focus. 2019 Dec 1;47(6):E9. doi: 10.3171/2019.9.FOCUS19605. Neurosurg Focus. 2019. PMID: 31786559 Review.
-
Reliability of intraoperative ultrasound in detecting tumor residual after brain diffuse glioma surgery: a systematic review and meta-analysis.Neurosurg Rev. 2020 Oct;43(5):1221-1233. doi: 10.1007/s10143-019-01160-x. Epub 2019 Aug 14. Neurosurg Rev. 2020. PMID: 31410683
Cited by
-
Enabling Navigation and Augmented Reality in the Sitting Position in Posterior Fossa Surgery Using Intraoperative Ultrasound.Cancers (Basel). 2024 May 23;16(11):1985. doi: 10.3390/cancers16111985. Cancers (Basel). 2024. PMID: 38893106 Free PMC article.
-
The Value of Intraoperative Ultrasound in Brain Surgery.Adv Tech Stand Neurosurg. 2024;50:185-199. doi: 10.1007/978-3-031-53578-9_6. Adv Tech Stand Neurosurg. 2024. PMID: 38592531
-
Effect of Nanoparticles of DOX and miR-125b on DNA Damage Repair in Glioma U251 Cells and Underlying Mechanisms.Molecules. 2022 Sep 21;27(19):6201. doi: 10.3390/molecules27196201. Molecules. 2022. PMID: 36234731 Free PMC article.
-
Intraoperative visualization of cerebral aneurysms using navigated 3D-ultrasound power-Doppler angiography.Acta Neurochir (Wien). 2024 Oct 19;166(1):417. doi: 10.1007/s00701-024-06310-9. Acta Neurochir (Wien). 2024. PMID: 39425799 Free PMC article.
-
Intraoperative Imaging and Optical Visualization Techniques for Brain Tumor Resection: A Narrative Review.Cancers (Basel). 2023 Oct 9;15(19):4890. doi: 10.3390/cancers15194890. Cancers (Basel). 2023. PMID: 37835584 Free PMC article. Review.
References
-
- Marko N.F., Weil R.J., Schroeder J.L., Lang F.F., Suki D., Sawaya R.E. Extent of Resection of Glioblastoma Revisited: Personalized Survival Modeling Facilitates More Accurate Survival Prediction and Supports a Maximum-Safe-Resection Approach to Surgery. J. Clin. Oncol. 2014;32:774. doi: 10.1200/JCO.2013.51.8886. - DOI - PMC - PubMed
-
- Wijnenga M.M.J., French P.J., Dubbink H.J., Dinjens W.N.M., Atmodimedjo P.N., Kros J.M., Smits M., Gahrmann R., Rutten G.-J., Verheul J.B. The Impact of Surgery in Molecularly Defined Low-Grade Glioma: An Integrated Clinical, Radiological, and Molecular Analysis. Neuro-Oncol. 2018;20:103–112. doi: 10.1093/neuonc/nox176. - DOI - PMC - PubMed
MeSH terms
LinkOut - more resources
Full Text Sources
Medical
