

Outcomes of Convalescent Plasma with Defined High versus Lower Neutralizing Antibody Titers against SARS-CoV-2 among Hospitalized Patients: CoronaVirus Inactivating Plasma (CoVIP) Study
- PMID: 36135380
- PMCID: PMC9601237
- DOI: 10.1128/mbio.01751-22
Outcomes of Convalescent Plasma with Defined High versus Lower Neutralizing Antibody Titers against SARS-CoV-2 among Hospitalized Patients: CoronaVirus Inactivating Plasma (CoVIP) Study
Abstract
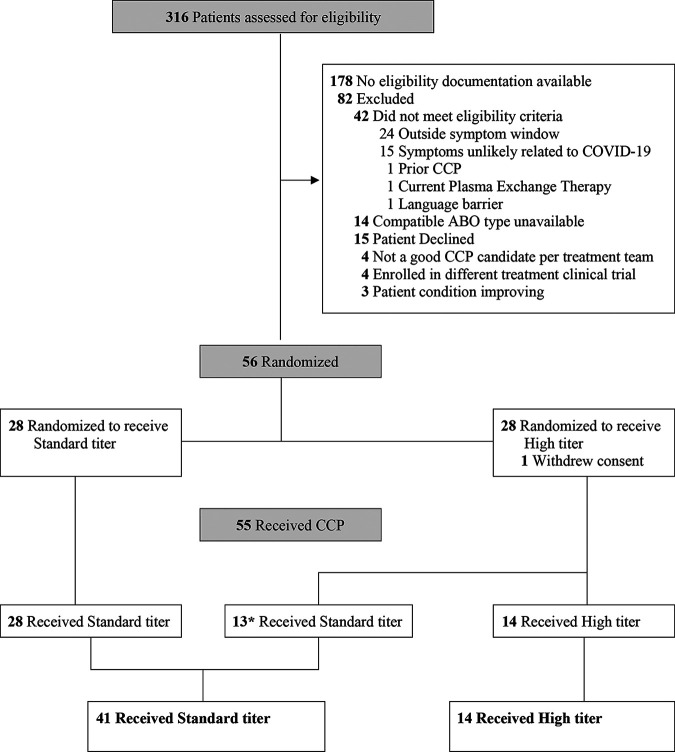
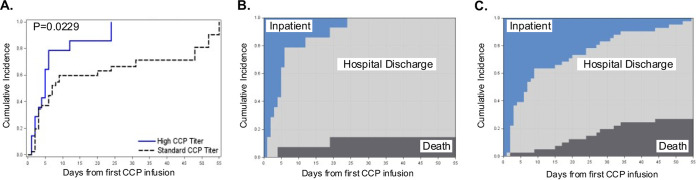
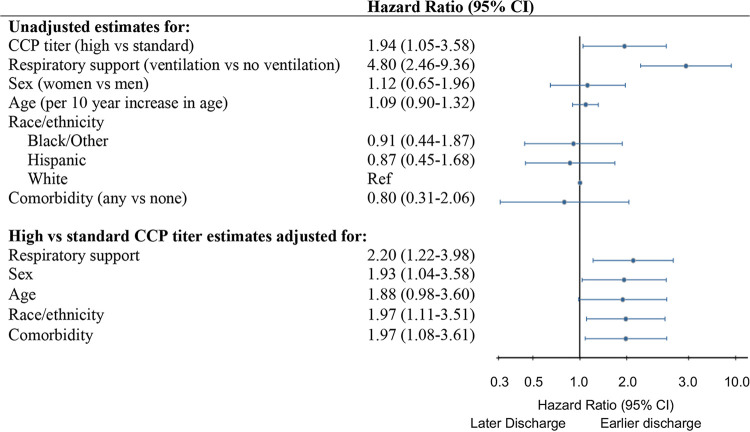
COVID-19 convalescent plasma (CCP) was an early and widely adopted putative therapy for severe COVID-19. Results from randomized control trials and observational studies have failed to demonstrate a clear therapeutic role for CCP for severe acute respiratory syndrome coronavirus 2 (SARS-CoV-2) infection. Underlying these inconclusive findings is a broad heterogeneity in the concentrations of neutralizing antibodies (nAbs) between different CCP donors. We conducted this study to evaluate the effectiveness and safety of nAb titer-defined CCP in adults admitted to an academic referral hospital. Patients positive by a SARS-CoV-2 nucleic acid amplification test and with symptoms for <10 days were eligible. Participants received either CCP with nAb titers of >1:640 (high-titer group) or ≥1:160 to 1:640 (standard-titer group) in addition to standard of care treatments. The primary clinical outcome was time to hospital discharge, with mortality and respiratory support evaluated as secondary outcomes. Adverse events were contrasted by CCP titer. Between 28 August and 4 December 2020, 316 participants were screened, and 55 received CCP, with 14 and 41 receiving high- versus standard-titer CCP, respectively. Time to hospital discharge was shorter among participants receiving high- versus standard-titer CCP, accounting for death as a competing event (hazard ratio, 1.94; 95% confidence interval [CI], 1.05 to 3.58; Gray's P = 0.02). Severe adverse events (SAEs) (≥grade 3) occurred in 4 (29%) and 23 (56%) of participants receiving the high versus standard titer, respectively, by day 28 (risk ratio, 0.51; 95% CI, 0.21 to 1.22; Fisher's P = 0.12). There were no observed treatment-related AEs. (This study has been registered at ClinicalTrials.gov under registration no. NCT04524507). IMPORTANCE In this study, in a high-risk population of patients admitted for COVID-19, we found an earlier time to hospital discharge among participants receiving CCP with nAb titers of >1:640 compared with participants receiving CCP with a lower nAb titer and no CCP-related AEs. The significance of our research is in identifying a dose response of CCP and clinical outcomes based on nAb titer. Although limited by a small study size, these findings support further study of high-nAb-titer CCP defined as >1:640 in the treatment of COVID-19.
Keywords: SARS-CoV-2; antibodies; convalescent plasma; coronavirus; immunology; neutralizing antibodies.
Conflict of interest statement
The authors declare a conflict of interest. D.M.M. has provided consultancy to Merck outside of this work, and owns common stock in Gilead Sciences. All other authors have no conflicts of interest to declare.
Figures
Comment in
-
Commentary on "Outcomes of Convalescent Plasma with Defined High versus Lower Neutralizing Antibody Titers against SARS-CoV-2 among Hospitalized Patients: CoronaVirus Inactivating Plasma (CoVIP) Study".mBio. 2022 Dec 20;13(6):e0265322. doi: 10.1128/mbio.02653-22. Epub 2022 Oct 31. mBio. 2022. PMID: 36314790 Free PMC article.
References
-
- O'Donnell MR, Grinsztejn B, Cummings MJ, Justman JE, Lamb MR, Eckhardt CM, Philip NM, Cheung YK, Gupta V, João E, Pilotto JH, Diniz MP, Cardoso SW, Abrams D, Rajagopalan KN, Borden SE, Wolf A, Sidi LC, Vizzoni A, Veloso VG, Bitan ZC, Scotto DE, Meyer BJ, Jacobson SD, Kantor A, Mishra N, Chauhan LV, Stone EF, Dei Zotti F, La Carpia F, Hudson KE, Ferrara SA, Schwartz J, Stotler BA, Lin WW, Wontakal SN, Shaz B, Briese T, Hod EA, Spitalnik SL, Eisenberger A, Lipkin WI. 2021. A randomized double-blind controlled trial of convalescent plasma in adults with severe COVID-19. J Clin Invest 131:e150646. doi: 10.1172/JCI150646. - DOI - PMC - PubMed
-
- Bégin P, Callum J, Jamula E, Cook R, Heddle NM, Tinmouth A, Zeller MP, Beaudoin-Bussières G, Amorim L, Bazin R, Loftsgard KC, Carl R, Chassé M, Cushing MM, Daneman N, Devine DV, Dumaresq J, Fergusson DA, Gabe C, Glesby MJ, Li N, Liu Y, McGeer A, Robitaille N, Sachais BS, Scales DC, Schwartz L, Shehata N, Turgeon AF, Wood H, Zarychanski R, Finzi A, Arnold DM, CONCOR-1 Study Group . 2021. Convalescent plasma for hospitalized patients with COVID-19: an open-label, randomized controlled trial. Nat Med 27:2012–2024. doi: 10.1038/s41591-021-01488-2. - DOI - PMC - PubMed
-
- Avendano-Sola C, Ramos-Martínez A, Muñez-Rubio E, Ruiz-Antorán B, Malo de Molina R, Torres F, Fernández-Cruz A, Calderón-Parra J, Payares-Herrera C, Díaz de Santiago A, Romera-Martínez I, Pintos I, Lora-Tamayo J, Mancheño-Losa M, Paciello ML, Martínez-González AL, Vidán-Estévez J, Nuñez-Orantos MJ, Saez-Serrano MI, Porras-Leal ML, Jarilla-Fernández MC, Villares P, de Oteyza JP, Ramos-Garrido A, Blanco L, Madrigal-Sánchez ME, Rubio-Batllés M, Velasco-Iglesias A, Paño-Pardo JR, Moreno-Chulilla JA, Muñiz-Díaz E, Casas-Flecha I, Pérez-Olmeda M, García-Pérez J, Alcamí J, Bueno JL, Duarte RF, ConPlas-19 Study Group . 2021. A multicenter randomized open-label clinical trial for convalescent plasma in patients hospitalized with COVID-19 pneumonia. J Clin Invest 131:e152740. doi: 10.1172/JCI152740. - DOI - PMC - PubMed
Publication types
MeSH terms
Substances
Associated data
Grants and funding
LinkOut - more resources
Full Text Sources
Other Literature Sources
Medical
Miscellaneous
