

Sex differences in arterial hypertension
- PMID: 36136303
- PMCID: PMC9726450
- DOI: 10.1093/eurheartj/ehac470
Sex differences in arterial hypertension
Abstract
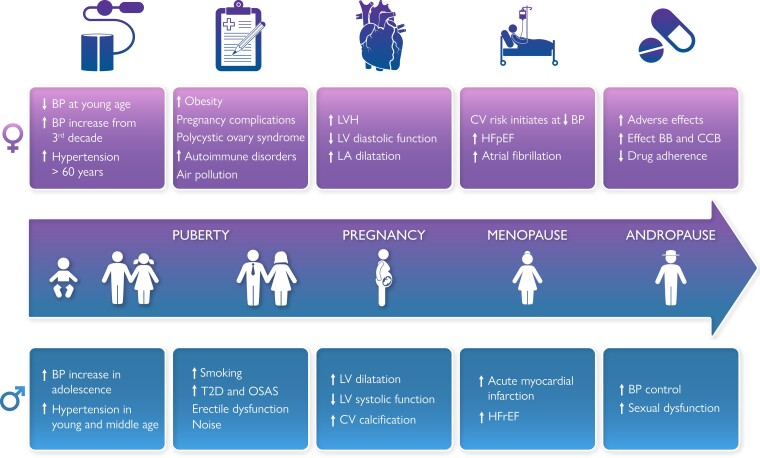
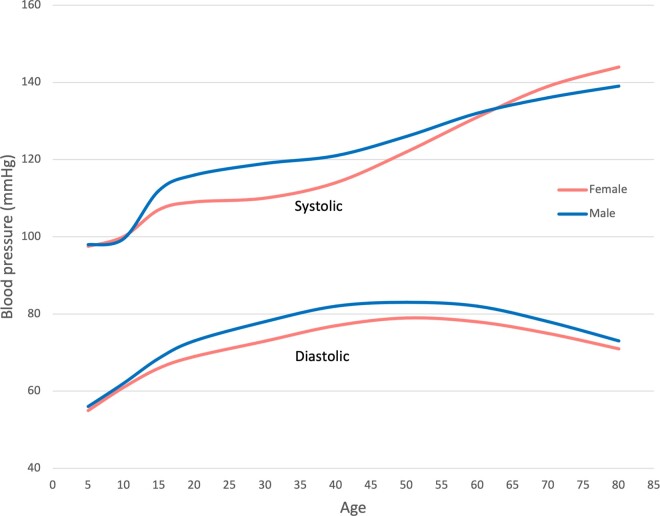
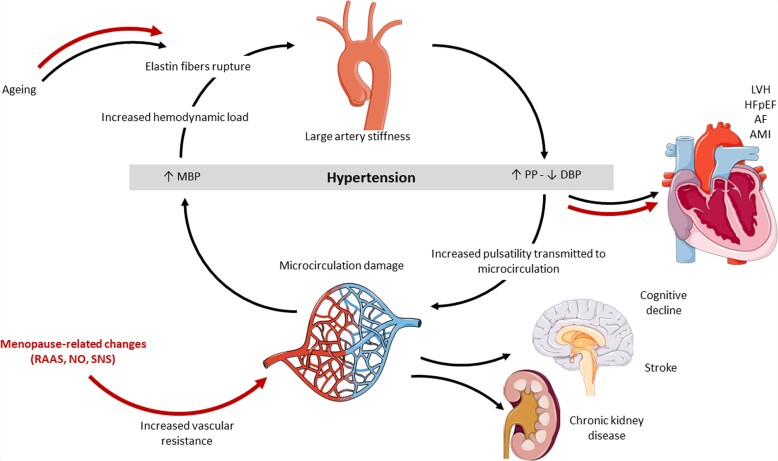
There is strong evidence that sex chromosomes and sex hormones influence blood pressure (BP) regulation, distribution of cardiovascular (CV) risk factors and co-morbidities differentially in females and males with essential arterial hypertension. The risk for CV disease increases at a lower BP level in females than in males, suggesting that sex-specific thresholds for diagnosis of hypertension may be reasonable. However, due to paucity of data, in particularly from specifically designed clinical trials, it is not yet known whether hypertension should be differently managed in females and males, including treatment goals and choice and dosages of antihypertensive drugs. Accordingly, this consensus document was conceived to provide a comprehensive overview of current knowledge on sex differences in essential hypertension including BP development over the life course, development of hypertension, pathophysiologic mechanisms regulating BP, interaction of BP with CV risk factors and co-morbidities, hypertension-mediated organ damage in the heart and the arteries, impact on incident CV disease, and differences in the effect of antihypertensive treatment. The consensus document also highlights areas where focused research is needed to advance sex-specific prevention and management of hypertension.
Keywords: Adverse events; Blood Pressure regulators; Cardiovascular disease; Hypertension; Hypertension-mediated organ damage; Pharmacological treatment; Sex; Sex hormones.
© The Author(s) 2022. Published by Oxford University Press on behalf of European Society of Cardiology.
Conflict of interest statement
Conflict of interest: E.G.: Bayer Health, NOKLUS, Fürst laboratories; I.S. Amgen, Astra Zeneca, Daiichi Sankio, Medtronic, Merck Sharpe & Dohme, Novartis, Recordati, Sanofi and Servier; SB Daiichi Sankyo; Merck, Sanofi, Menarini and Servier; C.B. Menarini Corporate, Servier, Novo Nordisk and Novartis; R.M.B. Medtronic; C.C.: none; V.C.: none; F.D.: none; M.F.: none; T.K.: TK Medtronics, and ReCor Medical; M.L.L.: Bayer Health, Sanofi, Bristol Myers Squibb and Pfizer; AHEMM: Organon, Novartis, Abbott and Omron; F.M.: Medtronic, ReCor Medical, Astra-Zeneca, Bayer, Boerhringer-Ingelheim, Medtronic, Merck and ReCor Medical; A.S.M.: Servier and SCAI; T.M.: none; G.P.: none; G.d.S.: none.
Figures
References
-
- GBD 2013 Risk Factors Collaborators, Forouzanfar MH, Alexander L, Anderson HR, Bachman VF, Biryukov S, et al. Global, regional, and national comparative risk assessment of 79 behavioural, environmental and occupational, and metabolic risks or clusters of risks in 188 countries, 1990-2013: a systematic analysis for the global burden of disease study 2013. Lancet 2015;386:2287–2323. - PMC - PubMed
-
- Bartz D, Chitnis T, Kaiser UB, Rich-Edwards JW, Rexrode KM, Pennell PB, et al. Clinical advances in sex- and gender-informed medicine to improve the health of all: A review. JAMA Intern Med 2020;180:574–583. - PubMed
-
- Yang BY, Qian Z, Howard SW, Vaughn MG, Fan SJ, Liu KK, et al. Global association between ambient air pollution and blood pressure: a systematic review and meta-analysis. Environ Pollut 2018;235:576–588. - PubMed
