

Health Care Personnel Exposures to Subsequently Laboratory-Confirmed Monkeypox Patients - Colorado, 2022
- PMID: 36136939
- PMCID: PMC9531564
- DOI: 10.15585/mmwr.mm7138e2
Health Care Personnel Exposures to Subsequently Laboratory-Confirmed Monkeypox Patients - Colorado, 2022
Abstract
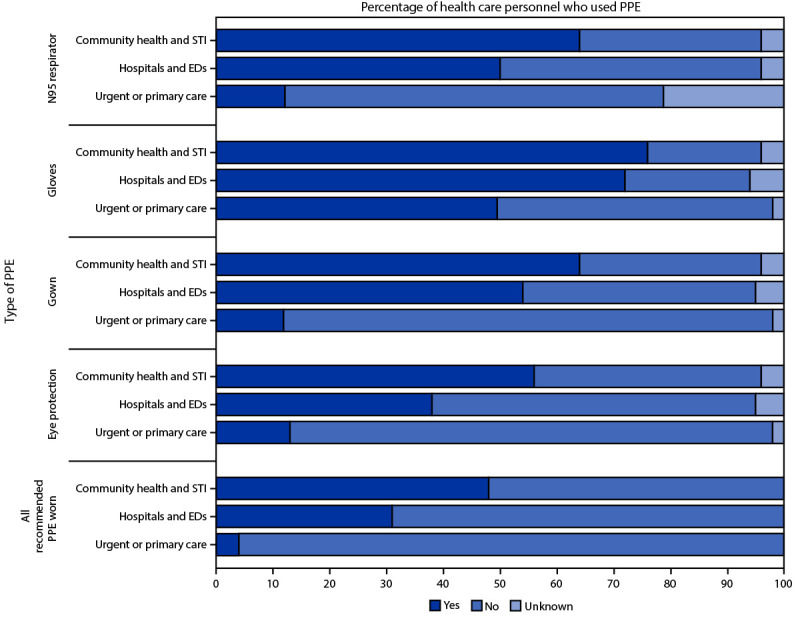
The risk for monkeypox transmission to health care personnel (HCP) caring for symptomatic patients is thought to be low but has not been thoroughly assessed in the context of the current global outbreak (1). Monkeypox typically spreads through close physical (often skin-to-skin) contact with lesions or scabs, body fluids, or respiratory secretions of a person with an active monkeypox infection. CDC currently recommends that HCP wear a gown, gloves, eye protection, and an N95 (or higher-level) respirator while caring for patients with suspected or confirmed monkeypox to protect themselves from infection† (1,2). The Colorado Department of Public Health and Environment (CDPHE) evaluated HCP exposures and personal protective equipment (PPE) use in health care settings during care of patients who subsequently received a diagnosis of Orthopoxvirus infection (presumptive monkeypox determined by a polymerase chain reaction [PCR] DNA assay) or monkeypox (real-time PCR assay and genetic sequencing performed by CDC). During May 1-July 31, 2022, a total of 313 HCP interacted with patients with subsequently diagnosed monkeypox infections while wearing various combinations of PPE; 23% wore all recommended PPE during their exposures. Twenty-eight percent of exposed HCP were considered to have had high- or intermediate-risk exposures and were therefore eligible to receive postexposure prophylaxis (PEP) with the JYNNEOS vaccine§; among those, 48% (12% of all exposed HCP) received the vaccine. PPE use varied by facility type: HCP in sexually transmitted infection (STI) clinics and community health centers reported the highest adherence to recommended PPE use, and primary and urgent care settings reported the lowest adherence. No HCP developed a monkeypox infection during the 21 days after exposure. These results suggest that the risk for transmission of monkeypox in health care settings is low. Infection prevention training is important in all health care settings, and these findings can guide future updates to PPE recommendations and risk classification in health care settings.
Conflict of interest statement
All authors have completed and submitted the International Committee of Medical Journal Editors form for disclosure of potential conflicts of interest. Rachel K. Herlihy reports support from the Council of State and Territorial Epidemiologists for travel to their annual conference. No other potential conflicts of interest were disclosed.
Figures
References
MeSH terms
LinkOut - more resources
Full Text Sources
Medical
Miscellaneous
