

Arterial Spin-Labeling Perfusion Metrics in Pediatric Posterior Fossa Tumor Surgery
- PMID: 36137658
- PMCID: PMC9575521
- DOI: 10.3174/ajnr.A7637
Arterial Spin-Labeling Perfusion Metrics in Pediatric Posterior Fossa Tumor Surgery
Abstract
Background and purpose: Pediatric posterior fossa tumors often present with hydrocephalus; postoperatively, up to 25% of patients develop cerebellar mutism syndrome. Arterial spin-labeling is a noninvasive means of quantifying CBF and bolus arrival time. The aim of this study was to investigate how changes in perfusion metrics in children with posterior fossa tumors are modulated by cerebellar mutism syndrome and hydrocephalus requiring pre-resection CSF diversion.
Materials and methods: Forty-four patients were prospectively scanned at 3 time points (preoperatively, postoperatively, and at 3-month follow-up) with single- and multi-inflow time arterial spin-labeling sequences. Regional analyses of CBF and bolus arrival time were conducted using coregistered anatomic parcellations. ANOVA and multivariable, linear mixed-effects modeling analysis approaches were used. The study was registered at clinicaltrials.gov (NCT03471026).
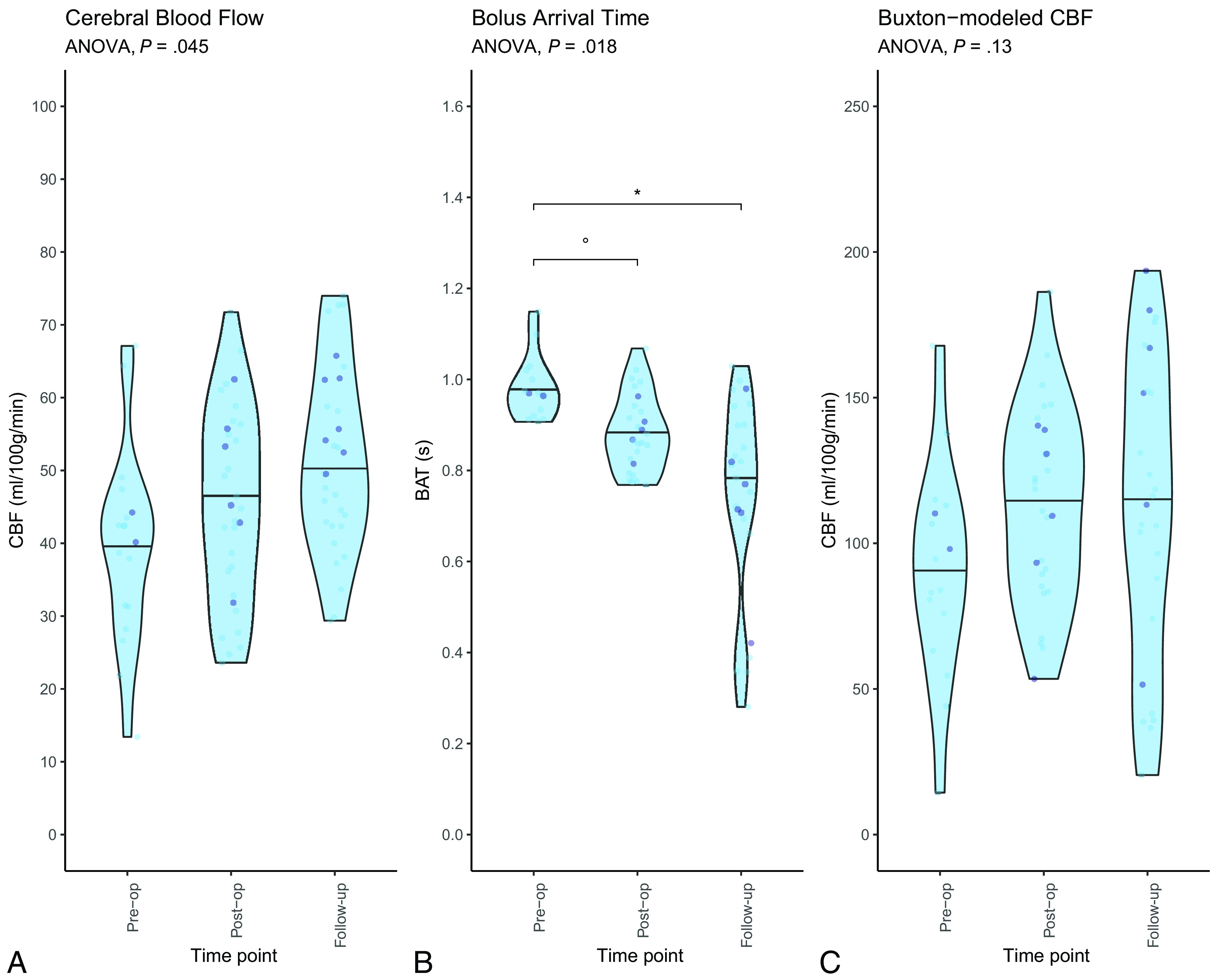
Results: CBF increased after tumor resection and at follow-up scanning (P = .045). Bolus arrival time decreased after tumor resection and at follow-up scanning (P = .018). Bolus arrival time was prolonged (P = .058) following the midline approach, compared with cerebellar hemispheric surgical approaches to posterior fossa tumors. Multivariable linear mixed-effects modeling showed that regional perfusion changes were more pronounced in the 6 children who presented with symptomatic obstructive hydrocephalus requiring pre-resection CSF diversion, with hydrocephalus lowering the baseline mean CBF by 20.5 (standard error, 6.27) mL/100g/min. Children diagnosed with cerebellar mutism syndrome (8/44, 18.2%) had significantly higher CBF at follow-up imaging than those who were not (P = .040), but no differences in pre- or postoperative perfusion parameters were seen.
Conclusions: Multi-inflow time arterial spin-labeling shows promise as a noninvasive tool to evaluate cerebral perfusion in the setting of pediatric obstructive hydrocephalus and demonstrates increased CBF following resolution of cerebellar mutism syndrome.
© 2022 by American Journal of Neuroradiology.
Figures


References
-
- Kerscher S, Schoning M, Schuhmann M. Raised ICP decreases cerebral blood flow volume in pediatric patients. In: Proceedings of the Annual Meeting of the International Society for Paediatric Neurosurgery, Birmingham, UK. October 20–24, 2019
Publication types
MeSH terms
Substances
Associated data
LinkOut - more resources
Full Text Sources
Medical