

Temporal order of clinical and biomarker changes in familial frontotemporal dementia
- PMID: 36138153
- PMCID: PMC9951811
- DOI: 10.1038/s41591-022-01942-9
Temporal order of clinical and biomarker changes in familial frontotemporal dementia
Abstract
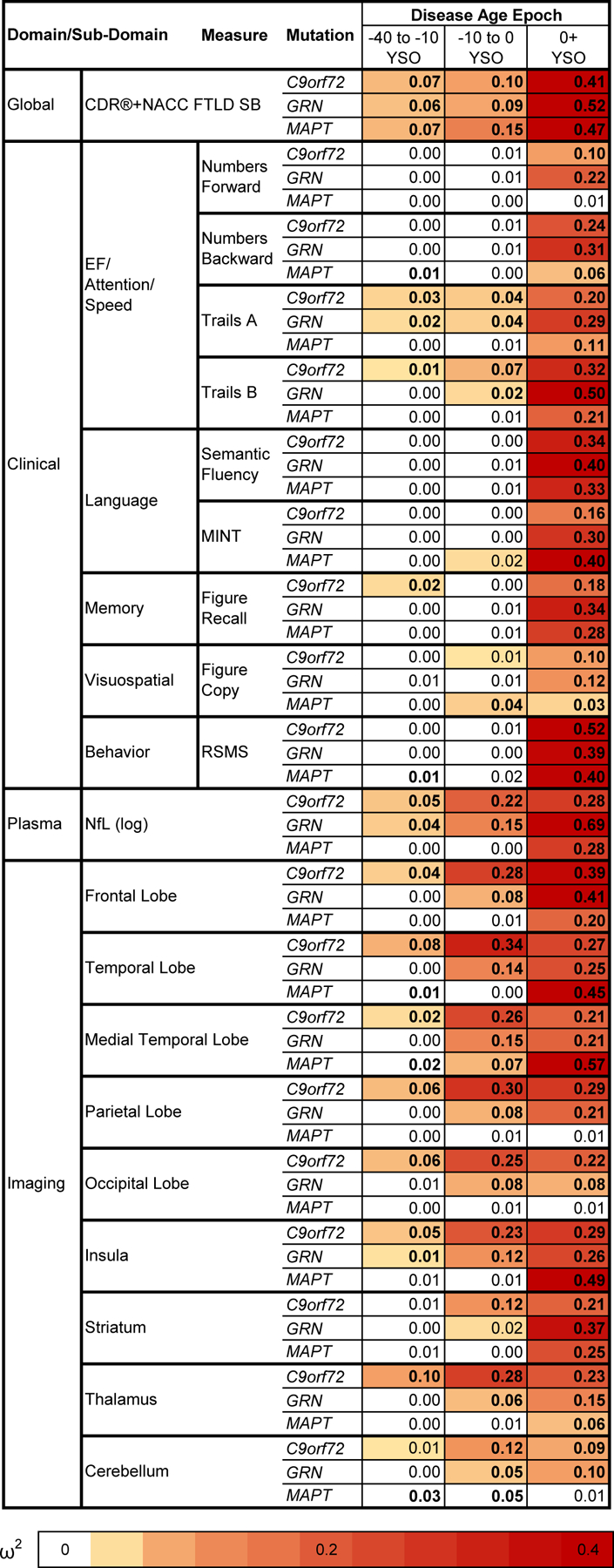
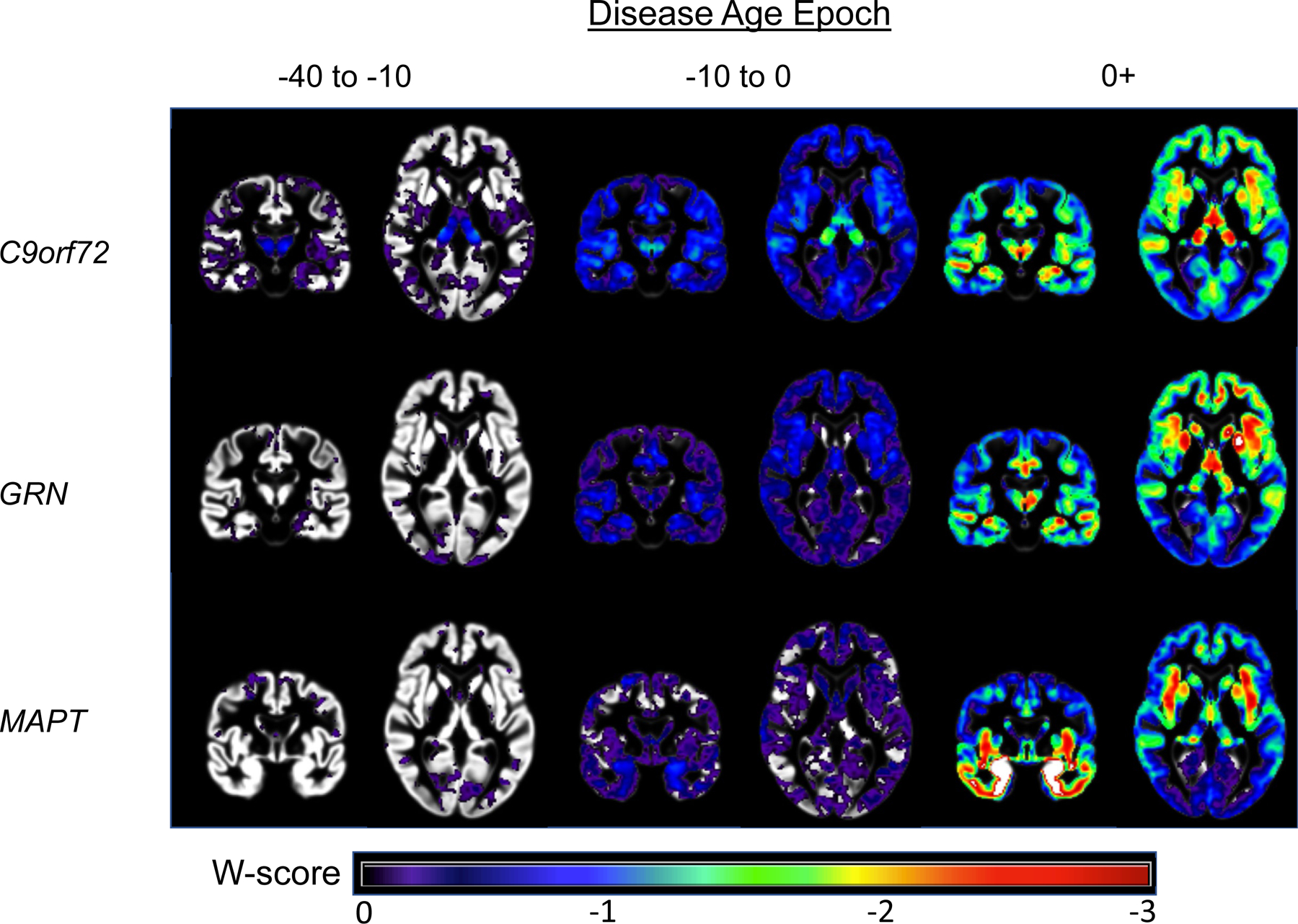
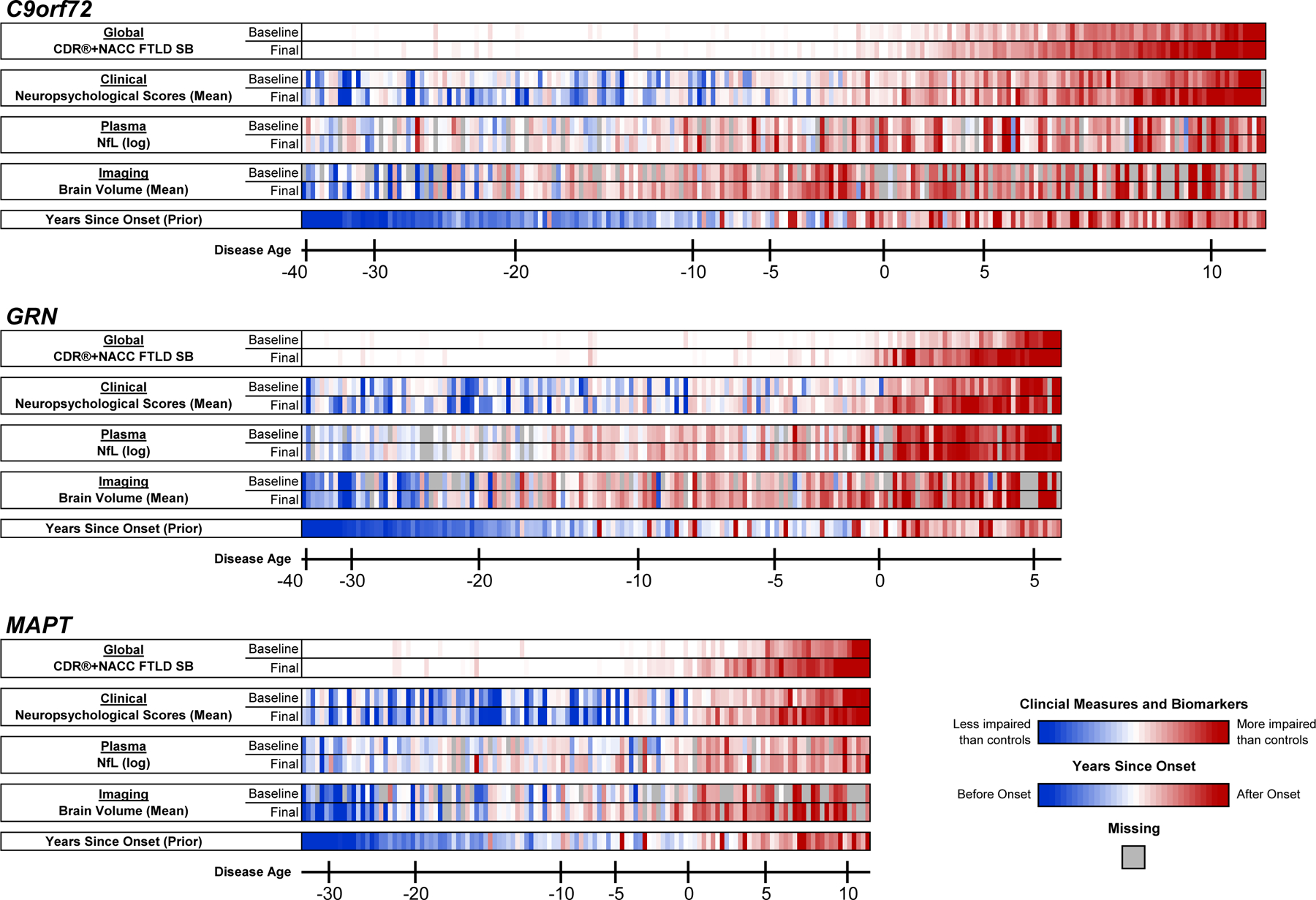
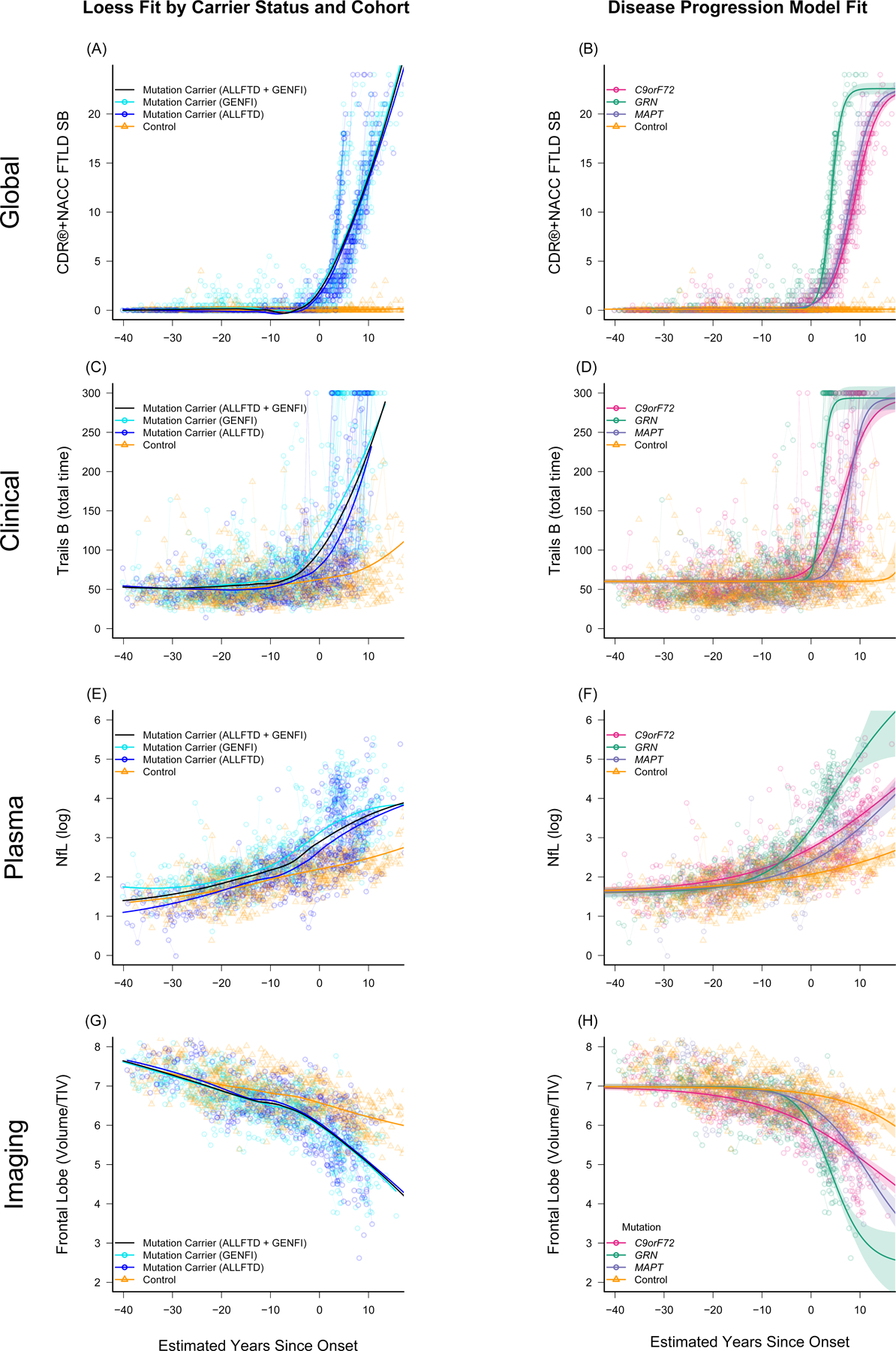
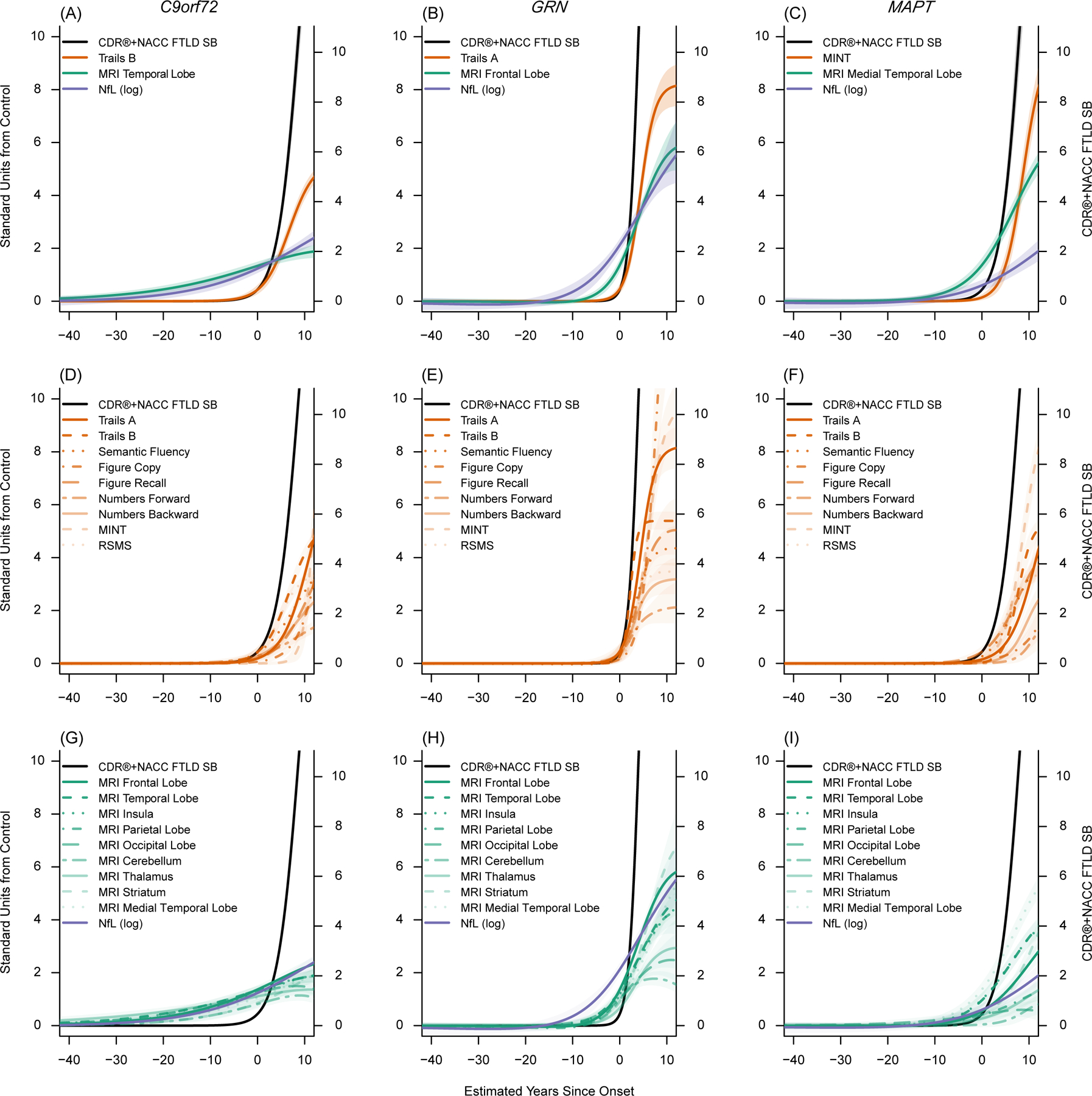
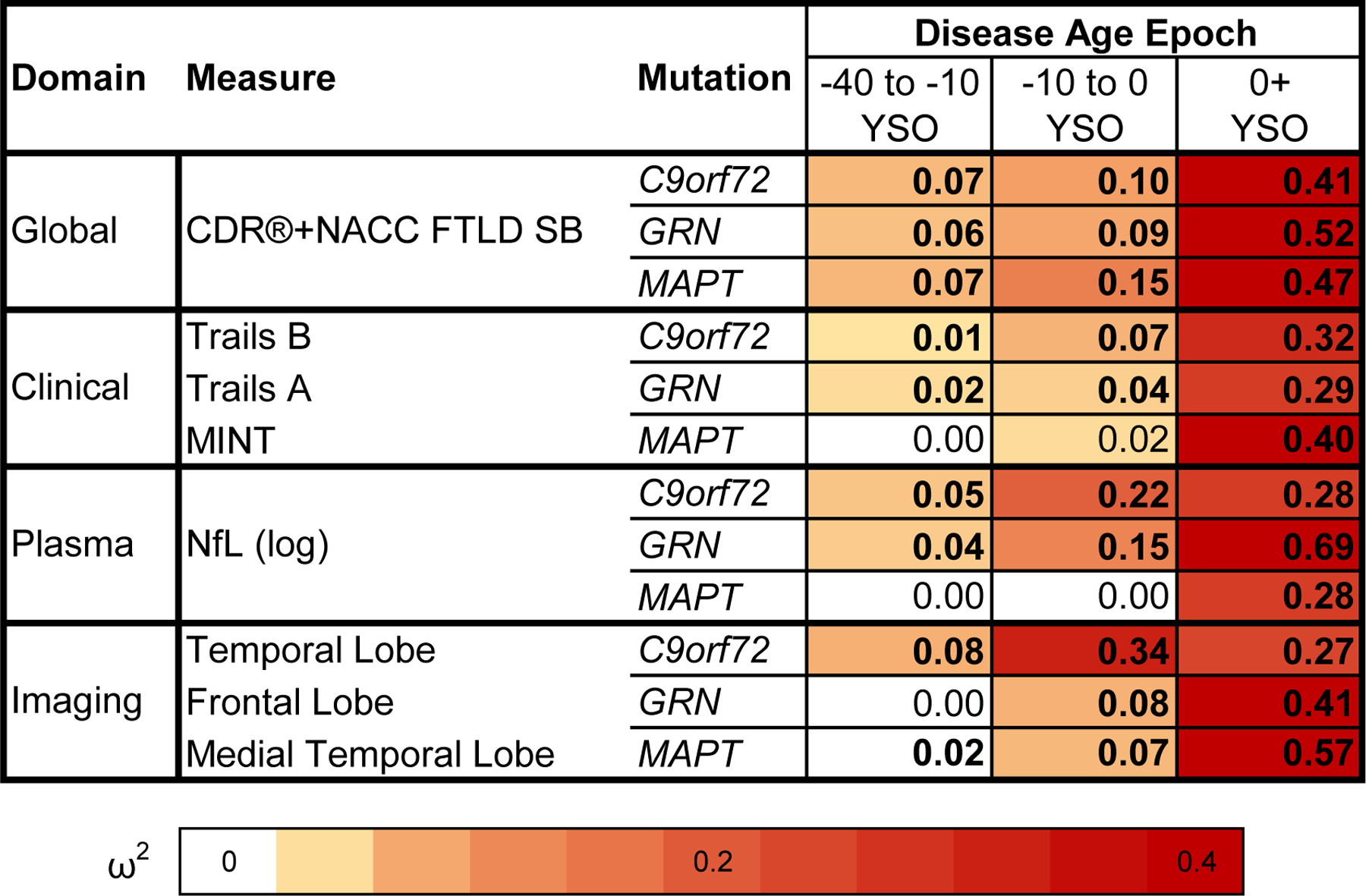
Unlike familial Alzheimer's disease, we have been unable to accurately predict symptom onset in presymptomatic familial frontotemporal dementia (f-FTD) mutation carriers, which is a major hurdle to designing disease prevention trials. We developed multimodal models for f-FTD disease progression and estimated clinical trial sample sizes in C9orf72, GRN and MAPT mutation carriers. Models included longitudinal clinical and neuropsychological scores, regional brain volumes and plasma neurofilament light chain (NfL) in 796 carriers and 412 noncarrier controls. We found that the temporal ordering of clinical and biomarker progression differed by genotype. In prevention-trial simulations using model-based patient selection, atrophy and NfL were the best endpoints, whereas clinical measures were potential endpoints in early symptomatic trials. f-FTD prevention trials are feasible but will likely require global recruitment efforts. These disease progression models will facilitate the planning of f-FTD clinical trials, including the selection of optimal endpoints and enrollment criteria to maximize power to detect treatment effects.
© 2022. The Author(s), under exclusive licence to Springer Nature America, Inc.
Figures
References
-
- Boeve BF, Boxer AL, Kumfor F, Pijnenburg Y & Rohrer JD Advances and controversies in frontotemporal dementia: diagnosis, biomarkers, and therapeutic considerations. Lancet. Neurol 21, 258–272 (2022). - PubMed
-
- Mercuri E et al. Nusinersen versus Sham Control in Later-Onset Spinal Muscular Atrophy. N. Engl. J. Med 378, 625–635 (2018). - PubMed
Methods-only references
Publication types
MeSH terms
Substances
Grants and funding
- K23 AG061253/AG/NIA NIH HHS/United States
- R01 AG058233/AG/NIA NIH HHS/United States
- K24 AG045333/AG/NIA NIH HHS/United States
- U24 AG072122/AG/NIA NIH HHS/United States
- P30 AG062422/AG/NIA NIH HHS/United States
- P01 AG019724/AG/NIA NIH HHS/United States
- R01 AG032306/AG/NIA NIH HHS/United States
- K12 HD001459/HD/NICHD NIH HHS/United States
- K23 AG059888/AG/NIA NIH HHS/United States
- BRC149/NS/MH/DH_/Department of Health/United Kingdom
- U54 NS092089/NS/NINDS NIH HHS/United States
- MR/T046015/1/MRC_/Medical Research Council/United Kingdom
- K23 AG073514/AG/NIA NIH HHS/United States
- BRC-1215-20014/DH_/Department of Health/United Kingdom
- L30 AG069301/AG/NIA NIH HHS/United States
- SUAG/092 G116768/MRC_/Medical Research Council/United Kingdom
- U24 AG021886/AG/NIA NIH HHS/United States
- MR/M008525/1/MRC_/Medical Research Council/United Kingdom
- RF1 AG029577/AG/NIA NIH HHS/United States
- R01 AG029577/AG/NIA NIH HHS/United States
- R01 AG038791/AG/NIA NIH HHS/United States
- U19 AG063911/AG/NIA NIH HHS/United States
- U01 AG016976/AG/NIA NIH HHS/United States
- MR/M023664/1/MRC_/Medical Research Council/United Kingdom
- P30 AG066509/AG/NIA NIH HHS/United States
- P30 AG072977/AG/NIA NIH HHS/United States
- P30 AG062677/AG/NIA NIH HHS/United States
- MR/K010395/1/MRC_/Medical Research Council/United Kingdom
- 220258 /WT_/Wellcome Trust/United Kingdom
- U01 AG045390/AG/NIA NIH HHS/United States
LinkOut - more resources
Full Text Sources
Miscellaneous
