

Aesthetic results in children with single suture craniosynostosis: proposal for a modified Whitaker classification
- PMID: 36138237
- PMCID: PMC9968690
- DOI: 10.1007/s00381-022-05678-2
Aesthetic results in children with single suture craniosynostosis: proposal for a modified Whitaker classification
Abstract
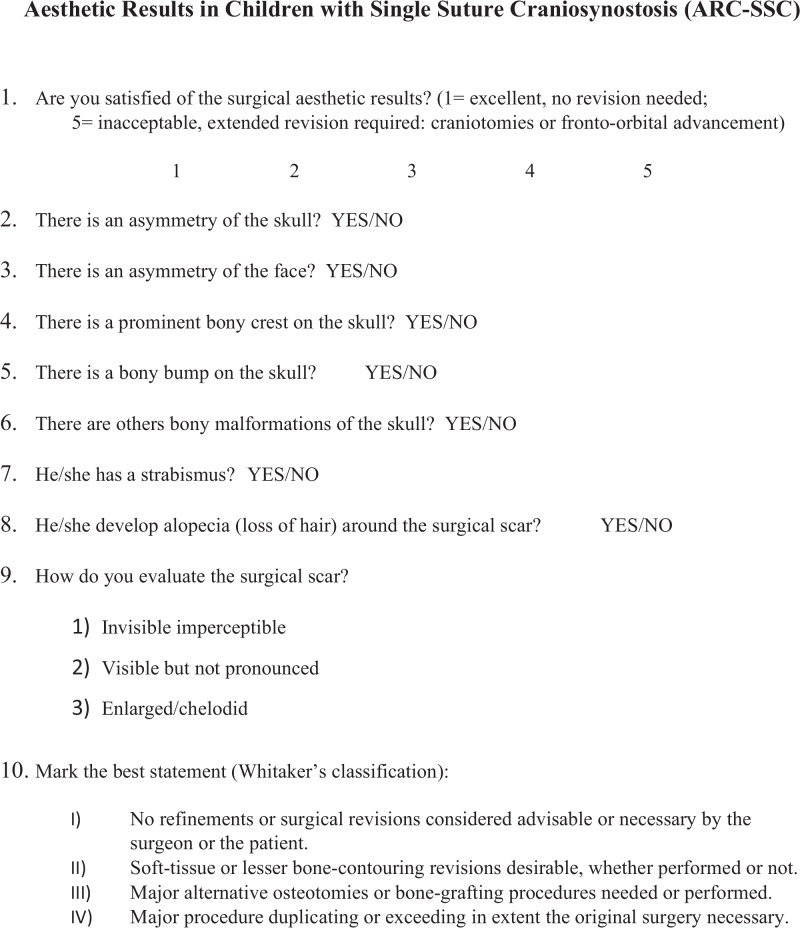
Objective: Aesthetic assessment after surgery for non-syndromic single suture craniosynostosis (SSC) is crucial. Surgeons' evaluation is generally based on Whitaker classification, while parental impression is generally neglected. The aim of this paper is to compare aesthetic perceptions of parents and surgeons after surgery for SSC, expressed by a 10-item questionnaire that complement Whitaker's classification.
Methods: The authors submitted a 10-item questionnaire integrating Whitaker's classification in order to evaluate the degree of satisfaction, the detailed aesthetics results and the need for surgical revision, to surgeons and parents of a consecutive series of patients operated for SSC between January 2007 and December 2018. The results were collected blindly.
Results: A total of 70 patients were included in the study. Scaphocephaly and trigonocephaly were the two most frequent craniosynostosis. Parents and surgeons general aesthetics evaluation and average rating for Whitaker's classification were 1.86 vs 1.67 (p = 0.69) and 1.19 vs 1.1 (p = 0.45) respectively. Parents' evaluation for scar perception and alopecia (p < 0.00001), the presence of bony crest (0.002), bony bump (p < 0.00001), or other bone irregularities (p = 0.02) are significantly worse when compared to surgeons' perception.
Conclusions: Parents seem to be more sensitive to the detection of some aesthetic anomalies and their opinion should not be neglected. The authors propose a modified Whitaker classification based on their results to better stratify the aesthetic outcome after surgery for SSC.
Keywords: Aesthetic result; Craniosynostosis; Surgery; Whitaker classification.
© 2022. The Author(s).
Conflict of interest statement
The authors declare no competing interests.
Figures




References
-
- Kabbani H, Raghuveer TS. Craniosynostosis. Am Fam Physician. 2004;69:2863–2870. - PubMed
MeSH terms
LinkOut - more resources
Full Text Sources
