

Mucinous cystic neoplasm of the liver with polypoid nodule prolapsing into the bile duct: a case report and review of literature
- PMID: 36138328
- PMCID: PMC9500141
- DOI: 10.1186/s40792-022-01511-9
Mucinous cystic neoplasm of the liver with polypoid nodule prolapsing into the bile duct: a case report and review of literature
Abstract
Background: Mucinous cystic neoplasm of the liver (MCN-L) is a rare cystic tumor as defined by the 2010 World Health Organization classification. MCN-L usually does not communicate with or grow into the bile duct. Herein, we present a rare case of MCN-L with a polypoid nodule protruding into the bile duct.
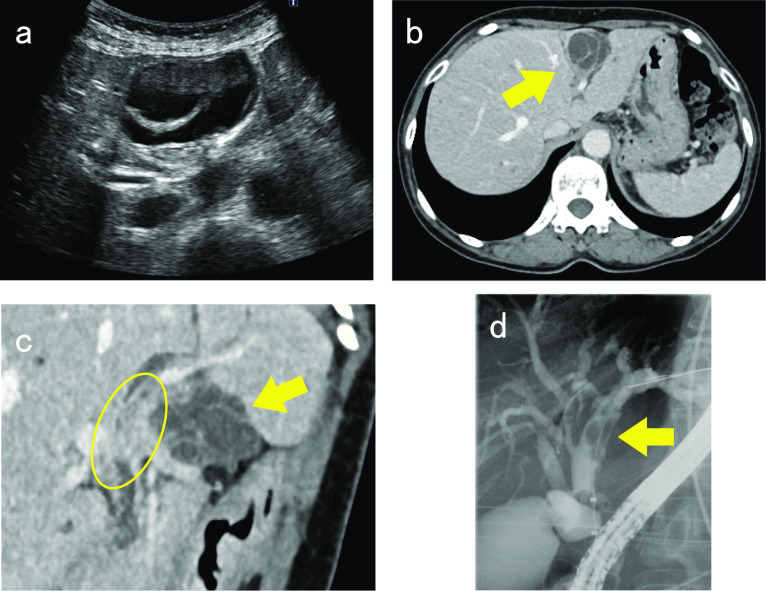
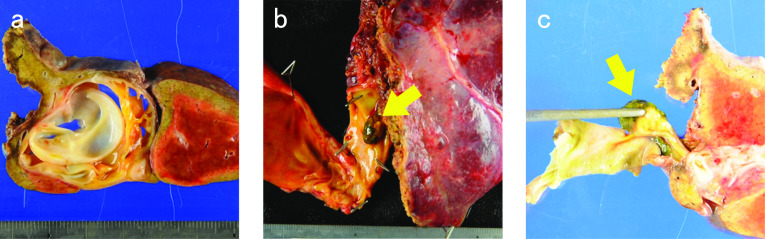
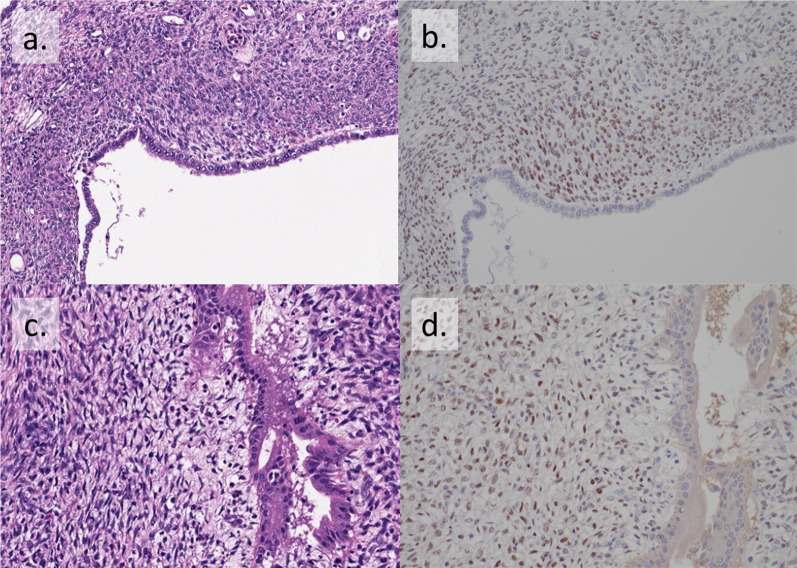
Case presentation: A 69-year-old woman was referred to our hospital for elevated serum liver enzyme levels and obstructive jaundice. The patient also complained of abdominal pain in the right hypochondriac region. Abdominal ultrasonography showed a cystic lesion in segment 4 (S4) of the liver. Computed tomography revealed a 4-cm multilocular cystic lesion with a thick wall and multiple septal formations, showing a cyst-in-cyst appearance in S4. Endoscopic retrograde cholangiography showed a contrast defect between the left hepatic duct and the common bile duct, which was suspected to be a nodular lesion in the bile duct. Bile cytology and biopsy of the nodular lesion showed no malignant findings. Based on these findings, the differential diagnosis in this patient included intraductal papillary neoplasm of the bile duct and MCN-L, which had malignant potential. The patient underwent left hemihepatectomy, including caudate lobe excision with bile duct resection and right hepatocholangiojejunostomy. Macroscopic findings showed a 40 × 29 mm multilocular cystic lesion with a polypoid nodule that protruded into the left intrahepatic bile duct. As an ovarian-like stroma was observed in both cystic and polypoid lesions microscopically, the histopathological diagnosis was MCN-L. The postoperative course was uneventful, and the patient was discharged 24 days after surgery. The patient is currently alive without recurrence 22 months after the surgery.
Conclusion: Although MCN-L rarely communicates with the bile duct, it is necessary to consider that MCN-L could grow into the bile duct, occasionally causing obstructive jaundice.
Keywords: Bile duct; Growth; Mucinous cystic neoplasm of the liver; Ovarian-like stroma.
© 2022. The Author(s).
Conflict of interest statement
The authors declare that they have no competing interests.
Figures
References
-
- Nakanuma Y, Curado M-P, Franceschi S, et al. WHO classification of tumours of the digestive system. 4. Lyon: WHO; 2010. pp. 217–224.
-
- Zen Y, Jang KT, Ahn S, Kim DH, Choi DW, Choi SH, et al. Intraductal papillary neoplasms and mucinous cystic neoplasms of the hepatobiliary system: demographic differences between Asian and Western populations, and comparison with pancreatic counterparts. Histopathology. 2014;65:164–173. doi: 10.1111/his.12378. - DOI - PubMed
-
- Kubota K, Nakanuma Y, Kondo F, Hachiya H, Miyazaki M, Nagino M, et al. Clinicopathological features and prognosis of mucin-producing bile duct tumor and mucinous cystic tumor of the liver: a multi-institutional study by the Japan Biliary Association. J Hepato-Biliary Pancreat Sci. 2014;21:176–185. doi: 10.1002/jhbp.23. - DOI - PubMed
LinkOut - more resources
Full Text Sources
Research Materials
