

Investigating the Impact of Ultra-Radical Surgery on Survival in Advanced Ovarian Cancer Using Population-Based Data in a Multicentre UK Study
- PMID: 36139523
- PMCID: PMC9497111
- DOI: 10.3390/cancers14184362
Investigating the Impact of Ultra-Radical Surgery on Survival in Advanced Ovarian Cancer Using Population-Based Data in a Multicentre UK Study
Abstract
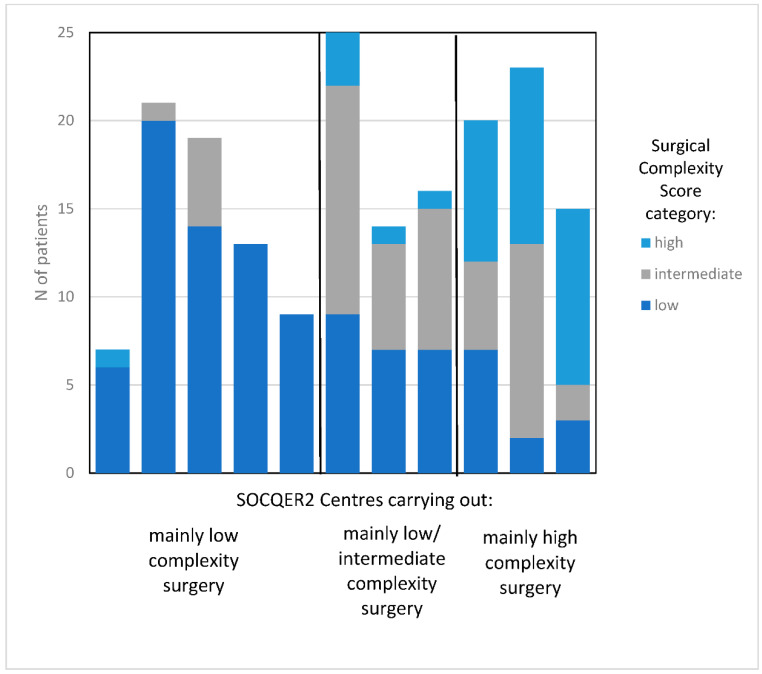
We investigated URS and impact on survival in whole patient cohorts with AOC treated within gynaecological cancer centres that participated in the previously presented SOCQER 2 study. National cancer registry datasets were used to identify FIGO Stage 3,4 and unknown stage patients from 11 cancer centres that had previously participated in the SOCQER2 study. Patient outcomes’ association with surgical ethos were evaluated using logistic regression and Cox proportional hazards. Centres were classified into three groups based on their surgical complexity scores (SCS); those practicing mainly low complexity, (5/11 centres with >70% low SCS procedures, 759 patients), mainly intermediate (3/11, 35−50% low SCS, 356 patients), or mainly high complexity surgery (3/11, >35% high SCS, 356 patients). Surgery rates were 43.2% vs. 58.4% vs. 60.9%. across mainly low, intermediate and high SCS centres, respectively, p < 0.001. Combined surgery and chemotherapy rates were 39.2% vs. 51.8% vs. 38.3% p < 0.000 across mainly low, intermediate and high complexity groups, respectively. Median survival was 23.1 (95% CI 19.0 to 27.2) vs. 22.0 (95% CI 17.6 to 26.3) vs. 17.9 months (95% CI 15.7 to 20.1), p = 0.043 in mainly high SCS, intermediate, and low SCS centres, respectively. In an age and deprivation adjusted model, compared to patients in the high SCS centres, patients in the low SCS group had an HR of 1.21 (95% CI 1.03 to 1.40) for death. Mainly high/intermediate SCS centres have significantly higher surgery rates and better survival at a population level. Centres that practice mainly low complexity surgery should change practice. This study provides support for the utilization of URS for patients with advanced OC.
Keywords: cytoreduction; ovarian cancer; population analysis; radical; surgical complexity; survival; ultra-radical.
Conflict of interest statement
The authors declare no conflict of interest.
Figures


References
-
- Fotopoulou C., Concin N., Planchamp F., Morice P., Vergote I., du Bois A., Querleu D. Quality indicators for advanced ovarian cancer surgery from the European Society of Gynaecological Oncology (ESGO): 2020 update. Int. J. Gynecol. Cancer. 2020;30:436–440. doi: 10.1136/ijgc-2020-001248. - DOI - PubMed
-
- Fotopoulou C., Hall M., Cruickshank D., Gabra H., Ganesan R., Hughes C., Kehoe S., Ledermann J., Morrison J., Naik R., et al. British Gynaecological Cancer Society (BGCS) epithelial ovarian/fallopian tube/primary peritoneal cancer guidelines: Recommendations for practice. Eur. J. Obstet. Gynecol. Reprod. Biol. 2017;213:123–139. doi: 10.1016/j.ejogrb.2017.04.016. - DOI - PubMed
-
- Armstrong D.K., Alvarez R.D., Bakkum-Gamez J.N., Barroilhet L., Behbakht K., Berchuck A., Chen L.M., Cristea M., DeRosa M., Eisenhauer E.L., et al. Ovarian Cancer, Version 2.2020, NCCN Clinical Practice Guidelines in Oncology. J. Natl. Compr. Canc. Netw. 2021;19:191–226. doi: 10.6004/jnccn.2021.0007. - DOI - PubMed
-
- Chi D.S., Franklin C.C., Levine D.A., Akselrod F., Sabbatini P., Jarnagin W.R., DeMatteo R., Poynor E.A., Abu-Rustum N.R., Barakat R.R. Improved optimal cytoreduction rates for stages IIIC and IV epithelial ovarian, fallopian tube, and primary peritoneal cancer: A change in surgical approach. Gynecol. Oncol. 2004;94:650–654. doi: 10.1016/j.ygyno.2004.01.029. - DOI - PubMed
LinkOut - more resources
Full Text Sources
