

Use of Deep Learning to Detect the Maternal Heart Rate and False Signals on Fetal Heart Rate Recordings
- PMID: 36140076
- PMCID: PMC9496277
- DOI: 10.3390/bios12090691
Use of Deep Learning to Detect the Maternal Heart Rate and False Signals on Fetal Heart Rate Recordings
Abstract
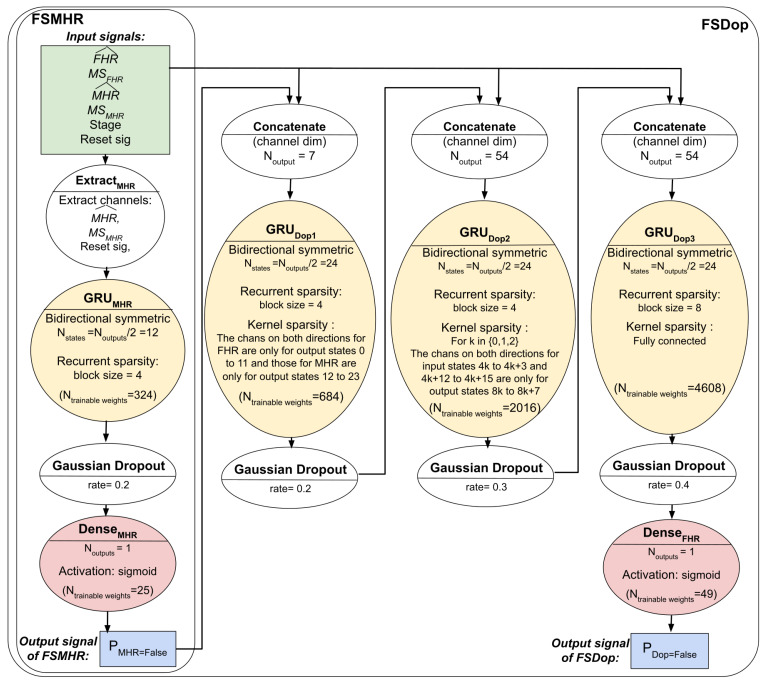
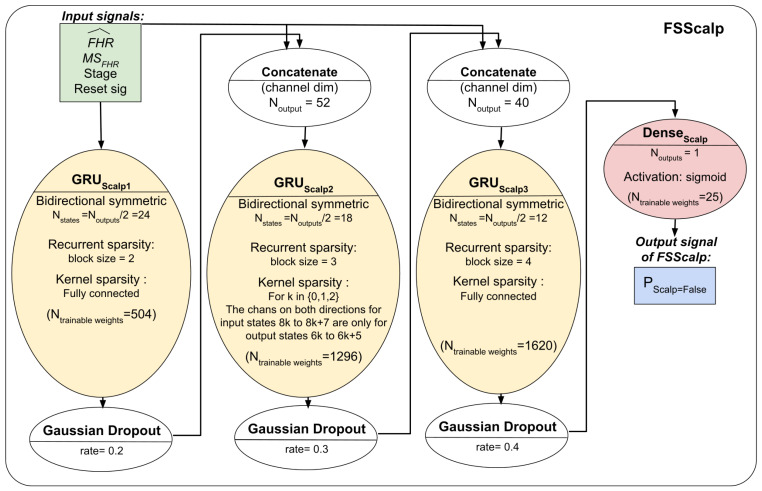
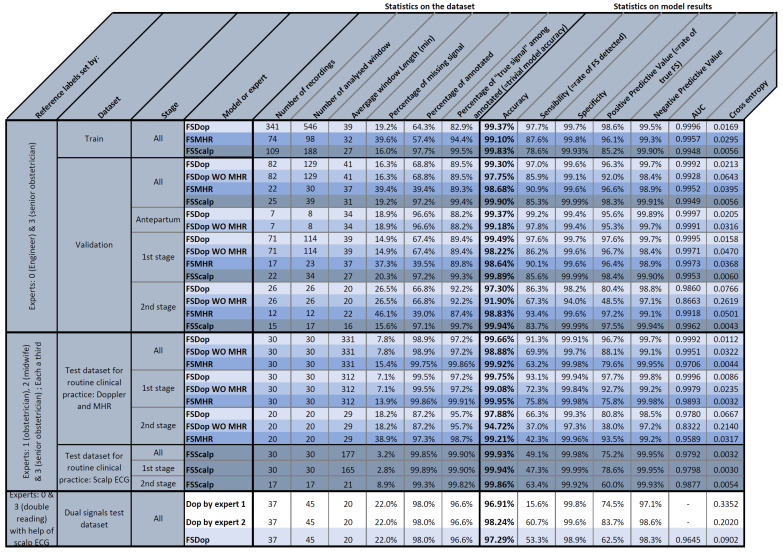
We have developed deep learning models for automatic identification of the maternal heart rate (MHR) and, more generally, false signals (FSs) on fetal heart rate (FHR) recordings. The models can be used to preprocess FHR data prior to automated analysis or as a clinical alert system to assist the practitioner. Three models were developed and used to detect (i) FSs on the MHR channel (the FSMHR model), (ii) the MHR and FSs on the Doppler FHR sensor (the FSDop model), and (iii) FSs on the scalp ECG channel (the FSScalp model). The FSDop model was the most useful because FSs are far more frequent on the Doppler FHR channel. All three models were based on a multilayer, symmetric, GRU, and were trained on data recorded during the first and second stages of delivery. The FSMHR and FSDop models were also trained on antepartum recordings. The training dataset contained 1030 expert-annotated periods (mean duration: 36 min) from 635 recordings. In an initial evaluation of routine clinical practice, 30 fully annotated recordings for each sensor type (mean duration: 5 h for MHR and Doppler sensors, and 3 h for the scalp ECG sensor) were analyzed. The sensitivity, positive predictive value (PPV) and accuracy were respectively 62.20%, 87.1% and 99.90% for the FSMHR model, 93.1%, 95.6% and 99.68% for the FSDop model, and 44.6%, 87.2% and 99.93% for the FSScalp model. We built a second test dataset with a more solid ground truth by selecting 45 periods (lasting 20 min, on average) on which the Doppler FHR and scalp ECG signals were recorded simultaneously. Using scalp ECG data, the experts estimated the true FHR value more reliably and thus annotated the Doppler FHR channel more precisely. The models achieved a sensitivity of 53.3%, a PPV of 62.4%, and an accuracy of 97.29%. In comparison, two experts (blinded to the scalp ECG data) respectively achieved a sensitivity of 15.7%, a PPV of 74.3%, and an accuracy of 96.91% and a sensitivity of 60.7%, a PPV of 83.5% and an accuracy of 98.24%. Hence, the models performed at expert level (better than one expert and worse than the other), although a well-trained expert with good knowledge of FSs could probably do better in some cases. The models and datasets have been included in the Fetal Heart Rate Morphological Analysis open-source MATLAB toolbox and can be used freely for research purposes.
Keywords: cardiotocogram; deep learning; fetal heart rate; gated recurrent unit; maternal heart rate.
Conflict of interest statement
The authors have no conflict of interest to declare.
Figures
References
-
- Health Encyclopedia. University of Rochester Medical Center; Rochester, NY, USA: [(accessed on 19 July 2022)]. External and Internal Heart Rate Monitoring of the Fetus. Available online: https://www.urmc.rochester.edu/encyclopedia/content.aspx?contenttypeid=9....
-
- Maternia A., Kupka T., Horoba K., Jezewski J., Martinek R., Wrobel J., Kahankova R., Czabanski R., Graczyk S. New Possibilities for Fetal Monitoring Using Unobtrusive Abdominal Electrocardiography; Proceedings of the 2019 MIXDES—26th International Conference “Mixed Design of Integrated Circuits and Systems”; Rzeszów, Poland. 27–29 June 2019; pp. 413–418. - DOI
-
- Lee K.J., Lee B. End-to-End Deep Learning Architecture for Separating Maternal and Fetal ECGs Using W-Net. IEEE Access. 2022;10:39782–39788. doi: 10.1109/ACCESS.2022.3166925. - DOI
-
- Odendaal H.J. False Interpretation of Fetal Heart Role Monitoring in Cases of Intra-Uterine Death. S. Afr. Med. J. 1976;50:1963–1965. - PubMed
MeSH terms
LinkOut - more resources
Full Text Sources
Other Literature Sources
Medical
